11 Temmuz 2012 Çarşamba
Trying To Conceive Over 40: Dealing With The Agonizing Wait From Month to Month
[Ljava.lang.String;@139d000c
10 Temmuz 2012 Salı
Adolescent Dating Violence: Are Public Schools Prepared to Deal with This Problem?
.lang.String;@52662385
9 Temmuz 2012 Pazartesi
Why Did Energy Expenditure Differ Between Diets in the Recent Study by Dr. Ludwig's Group?
To contact us Click HERE
As discussed in the previous post, a recent study by Dr. David Ludwig's group suggested that during weight maintenance following fat loss, eating a very low carbohydrate (VLC) diet led to a higher metabolic rate (energy expenditure) than eating a low-fat (LF) diet, with a low glycemic index (LGI) diet falling in between the two (1). The VLC diet was 30 percent protein, while the other two were 20 percent. It's important to note that these were three dietary patterns that differed in many ways, and contrary to claims that are being made in the popular media, the study was not designed to isolate the specific influence of protein, carbohydrate or fat on energy expenditure in this context.
Not only did the VLC diet lead to a higher total energy expenditure than the LF and LGI diets, the most remarkable finding is that it led to a higher resting energy expenditure. Basically, people on the VLC diet woke up in the morning burning more energy than people on the LGI diet, and people on the LGI diet woke up burning more than people on the LF diet. The VLC dieters burned 326 more calories than the LF dieters, and 200 more than the LGI dieters.
It's always tempting to view each new study in isolation, without considering the numerous studies that came before it, but in this case it's essential to see this study through a skeptical lens that places it into the proper scientific context. Previous studies have suggested that:
With that, let's see what could have accounted for the differences observed in Dr. Ludwig's study.
Was it Insulin?
I know it will be tempting to some people to attribute these results to changes in circulating insulin*. The hypothesis here is that lowering insulin increases energy expenditure. Let's see how plausible that is.
The first thing to point out is that the paper didn't actually report levels of fasting or meal-stimulated insulin, so we have no idea whether they differed, or if so, by how much. Most studies have shown that fasting insulin tends to be lower on diets that are very low in carbohydrate, but again this was not reported in the current study so all we can do is speculate. One would expect that the higher carbohydrate content of the low-fat diet in particular would lead to higher insulin after meals. However, the VLC diet was the highest in protein (30% vs. 20%), which also stimulates insulin release to a surprisingly large degree-- often more than an equivalent serving of carbohydrate (9). The point here is that we simply don't know how much insulin differed between the three groups.
The second, more important point is that lowering insulin levels does not appear to increase energy expenditure. The drug diazoxide, in addition to its effects in the brain and elsewhere, reduces both fasting and post-meal insulin secretion substantially (35-50%). In some but not all studies, diazoxide accelerates fat loss, and this may be related to its effects in a part of the brain called the hypothalamus
(10, 11, 12). When you give obese people diazoxide in conjunction with a low-calorie diet, it has no impact on energy expenditure, regardless of whether you look at the studies where it accelerated fat loss, or the ones where it didn't (13, 14). This suggests that when it works, it's because it reduces food intake.
Just to add more support to this idea, in free-living people, elevated insulin is associated with higher, not lower resting energy expenditure (15, 16). Insulin actually increases energy expenditure following a meal, at least in part via the brain, and so it is said to contribute to "diet-induced thermogenesis" (17). This is part of the reason why carbohydrate consumption is often associated with a higher post-meal energy expenditure than fat consumption (with protein being the highest, 18). It's worth noting that the difference in diet-induced thermogenesis between carbohydrate and fat is quite small.
Furthermore, it has been shown multiple times that on average, people with higher fasting insulin levels, and more insulin resistance, gain less fat over time than people with normal insulin levels (19). A recent study suggested that when you control for baseline fat mass however, this relationship disappears-- in other words, circulating insulin is not related to future fat gain (20). This is reminiscent of what we see in animal models, where a) increasing circulating insulin by making the liver insulin resistant does not cause fat gain (21), and b) preventing the increase in circulating insulin that normally occurs when they're given a fattening diet has no impact on the rate of fat gain (22). This shows that elevated circulating insulin is neither necessary nor sufficient to cause fat gain in animals, and suggests that the same is probably true in humans.
The overall point here is that insulin is not a compelling explanation for the effect they observed in this paper-- we need to look elsewhere.
Diet-induced Thermogenesis due to Increased Protein Intake
As mentioned above, protein increases energy expenditure following a meal (called 'diet-induced thermogenesis'), and differences in protein content between diets can result in differences in energy expenditure of up to 100 calories over the course of a day (23). The VLC diet was 30 percent protein, vs. 20 percent for the LGI and LF diets. This could account for a portion of the difference in total energy expenditure, although it can't account for the difference in resting energy expenditure because that's measured prior to eating.
Metabolic Inefficiency
The body contains and uses large quantities of protein, fat and carbohydrate. At macronutrient extremes, the body has to synthesize the missing macronutrient, and this is an energetically costly process. In the case of the VLC diet, participants' bodies would have had to make carbohydrate from amino acids and glycerol-- a process called gluconeogenesis. This uses energy, possibly accounting for a portion of the increased energy expenditure in that arm.
It would have been interesting to see a very low fat (10% or less) diet as a comparison group. It's possible that energy expenditure would have increased as participants approached the other end of macronutrient extremes.
How About Leptin and Insulin in the Brain?
One of the things I'd really like people to take away from my writing and talks is that where energy intake, energy expenditure, and body fatness are concerned, the brain is key. A particularly important system for fat mass regulation is the negative feedback loop between fat tissue and the brain that is completed by the hormone leptin. Leptin is by far the most important hormone for the regulation of body fatness in mammals. There are many things that influence food intake and energy expenditure, and some of these don't have a lot to do with leptin or physiology in general-- e.g. aunt Sally baked you a pie, or you're having drinks with friends, or you buy a dog and have to walk it twice a day. But leptin is the key hormone a circuit that does its best to regulate the balance between energy in, and energy out, and so it's always important to consider in cases like this.
As far as I know, the brain is the only organ that's capable of regulating energy expenditure, and it does so by controlling thyroid signaling, the HPA axis, the sympathetic/parasympathetic nervous systems, and physical movement. It has already been demonstrated that the metabolic response to fat loss in humans-- including the characteristic decline in energy expenditure per unit lean mass-- depends on the reduction in leptin that accompanies fat loss (24). The citation I just made was also in Dr. Ludwig's discussion section, and this is no coincidence! Although any explanation for Dr. Ludwig's finding is speculative at this point (duly acknowledged in the paper), leptin is a compelling possibility.
Leptin declined the most on the VLC diet, followed b the LGI diet, followed by LF. This doesn't tell us much about what's happening in the brain however, because we don't know how each diet affected leptin sensitivity. If changes in leptin signaling can account for the findings, then we would have to speculate that leptin sensitivity was increased in the VLC and LGI diets relative to the LF diet.
How the diets could have led to different leptin sensitivity in the brain is unknown. One intriguing possibility is that the decline in triglycerides improved leptin sensitivity. Dr. Bill Banks's research suggests that high circulating triglycerides impair leptin sensitivity in rodents (25). Dr. Banks is now at the University of Washington and I've had the pleasure of interacting with him a few times about this.
Another possibility is that the VLC diet led to improved insulin sensitivity in the brain. Insulin acts in the brain in a manner similar to leptin-- it suppresses food intake and increases energy expenditure, opposing fat gain (although to a much lesser degree than leptin, and the effect has historically been fickle). The VLC diet did appear to improve insulin sensitivity in the liver more than the other diets, so it's possible that it had such an effect in the brain as well.
Conclusion
It's always tempting to put the cart before the horse, and come to conclusions before we really know what's going on, but in this case all we can do is speculate. In my opinion, protein-induced thermogenesis, metabolic inefficiency, and alterations in the brain are the most likely explanations for the findings in this study, but we'll have to wait for future studies to see if this is true, and if so, why.
* Such as Gary Taubes's op-ed article in the NYT today. It proclaimed triumphantly that "a new study suggests that carbs, not calories, lead to weight gain". Back in reality-land, the study had nothing to do with what causes weight gain-- it was about fat loss maintenance in people who are already overweight (which are not metabolically analogous to pre-obese people as Taubes claims). There are numerous studies that compare the ability of fat and carbohydrate to actually cause fat gain, but these are inconvenient because they invariably show that 1) calorie intake is the dominant factor, and 2) fat is equally or more fattening than carbohydrate at a given calorie intake-- for example the study that concluded: "Excess dietary fat leads to greater fat accumulation than does excess dietary carbohydrate..." (26). In Dr. Ludwig's paper and the accompanying editorial in JAMA, they made no claims about carbohydrate being more fattening than fat, and they didn't even broach the topic, because Dr. Ludwig's study is not relevant to the question. I would love to see Dr. Ludwig set the record straight on this, but unfortunately most researchers don't fight back when their results are abused in the popular media.
Not only did the VLC diet lead to a higher total energy expenditure than the LF and LGI diets, the most remarkable finding is that it led to a higher resting energy expenditure. Basically, people on the VLC diet woke up in the morning burning more energy than people on the LGI diet, and people on the LGI diet woke up burning more than people on the LF diet. The VLC dieters burned 326 more calories than the LF dieters, and 200 more than the LGI dieters.
It's always tempting to view each new study in isolation, without considering the numerous studies that came before it, but in this case it's essential to see this study through a skeptical lens that places it into the proper scientific context. Previous studies have suggested that:
- The carbohydrate:fat ratio of the diet has little or no detectable impact on energy expenditure in people who are not trying to lose weight (2, 3).
- The carbohydrate:fat ratio of the diet has little or no detectable impact on energy expenditure in people who are being experimentally overfed, and if anything carbohydrate increases energy expenditure more than fat (4, 5).
- The carbohydrate:fat ratio of the diet has little or no detectable impact on energy expenditure during weight loss (6, 7, 8), and does not influence the rate of fat loss when calories are precisely controlled.
With that, let's see what could have accounted for the differences observed in Dr. Ludwig's study.
Was it Insulin?
I know it will be tempting to some people to attribute these results to changes in circulating insulin*. The hypothesis here is that lowering insulin increases energy expenditure. Let's see how plausible that is.
The first thing to point out is that the paper didn't actually report levels of fasting or meal-stimulated insulin, so we have no idea whether they differed, or if so, by how much. Most studies have shown that fasting insulin tends to be lower on diets that are very low in carbohydrate, but again this was not reported in the current study so all we can do is speculate. One would expect that the higher carbohydrate content of the low-fat diet in particular would lead to higher insulin after meals. However, the VLC diet was the highest in protein (30% vs. 20%), which also stimulates insulin release to a surprisingly large degree-- often more than an equivalent serving of carbohydrate (9). The point here is that we simply don't know how much insulin differed between the three groups.
The second, more important point is that lowering insulin levels does not appear to increase energy expenditure. The drug diazoxide, in addition to its effects in the brain and elsewhere, reduces both fasting and post-meal insulin secretion substantially (35-50%). In some but not all studies, diazoxide accelerates fat loss, and this may be related to its effects in a part of the brain called the hypothalamus
(10, 11, 12). When you give obese people diazoxide in conjunction with a low-calorie diet, it has no impact on energy expenditure, regardless of whether you look at the studies where it accelerated fat loss, or the ones where it didn't (13, 14). This suggests that when it works, it's because it reduces food intake.
Just to add more support to this idea, in free-living people, elevated insulin is associated with higher, not lower resting energy expenditure (15, 16). Insulin actually increases energy expenditure following a meal, at least in part via the brain, and so it is said to contribute to "diet-induced thermogenesis" (17). This is part of the reason why carbohydrate consumption is often associated with a higher post-meal energy expenditure than fat consumption (with protein being the highest, 18). It's worth noting that the difference in diet-induced thermogenesis between carbohydrate and fat is quite small.
Furthermore, it has been shown multiple times that on average, people with higher fasting insulin levels, and more insulin resistance, gain less fat over time than people with normal insulin levels (19). A recent study suggested that when you control for baseline fat mass however, this relationship disappears-- in other words, circulating insulin is not related to future fat gain (20). This is reminiscent of what we see in animal models, where a) increasing circulating insulin by making the liver insulin resistant does not cause fat gain (21), and b) preventing the increase in circulating insulin that normally occurs when they're given a fattening diet has no impact on the rate of fat gain (22). This shows that elevated circulating insulin is neither necessary nor sufficient to cause fat gain in animals, and suggests that the same is probably true in humans.
The overall point here is that insulin is not a compelling explanation for the effect they observed in this paper-- we need to look elsewhere.
Diet-induced Thermogenesis due to Increased Protein Intake
As mentioned above, protein increases energy expenditure following a meal (called 'diet-induced thermogenesis'), and differences in protein content between diets can result in differences in energy expenditure of up to 100 calories over the course of a day (23). The VLC diet was 30 percent protein, vs. 20 percent for the LGI and LF diets. This could account for a portion of the difference in total energy expenditure, although it can't account for the difference in resting energy expenditure because that's measured prior to eating.
Metabolic Inefficiency
The body contains and uses large quantities of protein, fat and carbohydrate. At macronutrient extremes, the body has to synthesize the missing macronutrient, and this is an energetically costly process. In the case of the VLC diet, participants' bodies would have had to make carbohydrate from amino acids and glycerol-- a process called gluconeogenesis. This uses energy, possibly accounting for a portion of the increased energy expenditure in that arm.
It would have been interesting to see a very low fat (10% or less) diet as a comparison group. It's possible that energy expenditure would have increased as participants approached the other end of macronutrient extremes.
How About Leptin and Insulin in the Brain?
One of the things I'd really like people to take away from my writing and talks is that where energy intake, energy expenditure, and body fatness are concerned, the brain is key. A particularly important system for fat mass regulation is the negative feedback loop between fat tissue and the brain that is completed by the hormone leptin. Leptin is by far the most important hormone for the regulation of body fatness in mammals. There are many things that influence food intake and energy expenditure, and some of these don't have a lot to do with leptin or physiology in general-- e.g. aunt Sally baked you a pie, or you're having drinks with friends, or you buy a dog and have to walk it twice a day. But leptin is the key hormone a circuit that does its best to regulate the balance between energy in, and energy out, and so it's always important to consider in cases like this.
As far as I know, the brain is the only organ that's capable of regulating energy expenditure, and it does so by controlling thyroid signaling, the HPA axis, the sympathetic/parasympathetic nervous systems, and physical movement. It has already been demonstrated that the metabolic response to fat loss in humans-- including the characteristic decline in energy expenditure per unit lean mass-- depends on the reduction in leptin that accompanies fat loss (24). The citation I just made was also in Dr. Ludwig's discussion section, and this is no coincidence! Although any explanation for Dr. Ludwig's finding is speculative at this point (duly acknowledged in the paper), leptin is a compelling possibility.
Leptin declined the most on the VLC diet, followed b the LGI diet, followed by LF. This doesn't tell us much about what's happening in the brain however, because we don't know how each diet affected leptin sensitivity. If changes in leptin signaling can account for the findings, then we would have to speculate that leptin sensitivity was increased in the VLC and LGI diets relative to the LF diet.
How the diets could have led to different leptin sensitivity in the brain is unknown. One intriguing possibility is that the decline in triglycerides improved leptin sensitivity. Dr. Bill Banks's research suggests that high circulating triglycerides impair leptin sensitivity in rodents (25). Dr. Banks is now at the University of Washington and I've had the pleasure of interacting with him a few times about this.
Another possibility is that the VLC diet led to improved insulin sensitivity in the brain. Insulin acts in the brain in a manner similar to leptin-- it suppresses food intake and increases energy expenditure, opposing fat gain (although to a much lesser degree than leptin, and the effect has historically been fickle). The VLC diet did appear to improve insulin sensitivity in the liver more than the other diets, so it's possible that it had such an effect in the brain as well.
Conclusion
It's always tempting to put the cart before the horse, and come to conclusions before we really know what's going on, but in this case all we can do is speculate. In my opinion, protein-induced thermogenesis, metabolic inefficiency, and alterations in the brain are the most likely explanations for the findings in this study, but we'll have to wait for future studies to see if this is true, and if so, why.
* Such as Gary Taubes's op-ed article in the NYT today. It proclaimed triumphantly that "a new study suggests that carbs, not calories, lead to weight gain". Back in reality-land, the study had nothing to do with what causes weight gain-- it was about fat loss maintenance in people who are already overweight (which are not metabolically analogous to pre-obese people as Taubes claims). There are numerous studies that compare the ability of fat and carbohydrate to actually cause fat gain, but these are inconvenient because they invariably show that 1) calorie intake is the dominant factor, and 2) fat is equally or more fattening than carbohydrate at a given calorie intake-- for example the study that concluded: "Excess dietary fat leads to greater fat accumulation than does excess dietary carbohydrate..." (26). In Dr. Ludwig's paper and the accompanying editorial in JAMA, they made no claims about carbohydrate being more fattening than fat, and they didn't even broach the topic, because Dr. Ludwig's study is not relevant to the question. I would love to see Dr. Ludwig set the record straight on this, but unfortunately most researchers don't fight back when their results are abused in the popular media.
Food allergy - top articles for June 2012
To contact us Click HERE
 Here are my suggestions for some of the top articles about food allergy for June 2012:
Here are my suggestions for some of the top articles about food allergy for June 2012:
"There is still misunderstanding in the general public about food allergy and how serious it can. Concerns that skin contact or inhalation might trigger severe food allergic reactions not supported - the vast majority happened from ingestion. Only 30% of severe food allergic reactions were appropriately treated with EpiPen, even when caregivers felt that was warranted. "Parents are surprised how quickly and effectively epinephrine works in food allergic reactions", yet many afraid to use it - USA Today http://goo.gl/0ZkxT
11% of children are being given the food they're allergic to on purpose, by caregivers, to see how they'll react http://buff.ly/Lc8hbi
Care for babies with food allergies lagging: study | Reuters http://buff.ly/Lxs083
The future of research in pediatric allergy: What should the focus be? (full text) http://goo.gl/9rh76
Food Allergy: Making an Accurate Diagnosis - 40-minute CME video with leading experts from Medscape http://goo.gl/CeDb2
Sesame Food Allergy may affect 0.1–0.2 % of the population, only one fatality has been reported http://goo.gl/oh1Y1
Evaluating a possible allergic reaction to beer is a difficult task - AAAAI Ask the Allergist http://goo.gl/LMsyW
FDA Sends Warning Letter to Pfizer Over EpiPen Ads - full text here: http://goo.gl/0ITDf
Egg white-specific serum IgG4/IgE ratio predicts outcome of food challenges http://goo.gl/r2t9t
Epinephrine in the treatment of anaphylaxis. Adult intramuscular dose is 0.3 to 0.5 ml of 1:1,000 concentration http://goo.gl/Qad6S
Nonallergen-specific experimental treatments for food allergy: Chinese Herbal Formula, Anti-IgE,
Probiotics and Prebiotics http://goo.gl/kKv69
Hygiene hypothesis may explain south/north geographical differences in prevalence of asthma and sarcoidosis http://goo.gl/FamUU
The articles were selected from my Twitter and Google Reader streams. Please feel free to send suggestions for articles to allergycases@gmail.com and you will receive acknowledgement in the next edition of this publication.
Image source: Wikipedia, GNU Free Documentation License.
Here are my suggestions for some of the top articles about food allergy for June 2012:"There is still misunderstanding in the general public about food allergy and how serious it can. Concerns that skin contact or inhalation might trigger severe food allergic reactions not supported - the vast majority happened from ingestion. Only 30% of severe food allergic reactions were appropriately treated with EpiPen, even when caregivers felt that was warranted. "Parents are surprised how quickly and effectively epinephrine works in food allergic reactions", yet many afraid to use it - USA Today http://goo.gl/0ZkxT
11% of children are being given the food they're allergic to on purpose, by caregivers, to see how they'll react http://buff.ly/Lc8hbi
Care for babies with food allergies lagging: study | Reuters http://buff.ly/Lxs083
The future of research in pediatric allergy: What should the focus be? (full text) http://goo.gl/9rh76
Food Allergy: Making an Accurate Diagnosis - 40-minute CME video with leading experts from Medscape http://goo.gl/CeDb2
Sesame Food Allergy may affect 0.1–0.2 % of the population, only one fatality has been reported http://goo.gl/oh1Y1
Evaluating a possible allergic reaction to beer is a difficult task - AAAAI Ask the Allergist http://goo.gl/LMsyW
FDA Sends Warning Letter to Pfizer Over EpiPen Ads - full text here: http://goo.gl/0ITDf
Egg white-specific serum IgG4/IgE ratio predicts outcome of food challenges http://goo.gl/r2t9t
Epinephrine in the treatment of anaphylaxis. Adult intramuscular dose is 0.3 to 0.5 ml of 1:1,000 concentration http://goo.gl/Qad6S
Nonallergen-specific experimental treatments for food allergy: Chinese Herbal Formula, Anti-IgE,
Probiotics and Prebiotics http://goo.gl/kKv69
Hygiene hypothesis may explain south/north geographical differences in prevalence of asthma and sarcoidosis http://goo.gl/FamUU
The articles were selected from my Twitter and Google Reader streams. Please feel free to send suggestions for articles to allergycases@gmail.com and you will receive acknowledgement in the next edition of this publication.
Image source: Wikipedia, GNU Free Documentation License.
Top articles in medicine in June 2012
To contact us Click HERE
 Here are my suggestions for some of the top articles in medicine in June 2012:
Here are my suggestions for some of the top articles in medicine in June 2012:
Cancer rates worldwide are expected to increase by 75% by 2030 http://goo.gl/Wu8i9
Zinc could be useful adjunct treatment in infants with probable serious bacterial infection - The Lancet http://goo.gl/Hgqs7
To screen or not to screen for prostate cancer? Fewer than 2% of Johns Hopkins doctors plan to follow the recommendations and stop ordering PSA screening - Lancet http://goo.gl/5Nkha
Dark chocolate could work as prevention therapy of cardiovascular disease - BMJ's exercise in wishful thinking: http://goo.gl/Om6kq
UV protection and sunscreens: What to tell patients - CCJM http://goo.gl/yhRH4 -- Related reading: How to avoid damaging ultraviolet light - CCJM launches "Patient Page" similar to JAMA http://bit.ly/MkL6Ae
NYTimes asks experts what they want from the future: "permanent sunblock that embeds in skin ~ Lasik eye surgery" ?! http://goo.gl/TnHZa -- Related: 32 Innovations Will Change Your Tomorrow - underwear with sensors tells how hard you’re working your quadriceps muscles http://goo.gl/EWRuX
Psoriasis: Evolving treatment for a complex disease - CCJM 2012 review, free full text http://goo.gl/Sc9Uy
Acute community-acquired bacterial meningitis in adults: CCJM 2012 review, free full text http://goo.gl/XKYQR
"Walmart clinics go live in the cloud": retail giant pushes healthcare providers to make diagnoses over the internet http://goo.gl/P51NW
A Single Inhalation of Laninamivir Works in Children With Influenza (study) http://goo.gl/BxgRs
Inhaled Hypertonic Saline (3%) mixed with albuterol reduces length of stay and admission rate for wheezing children http://goo.gl/g9cFH
College freshman at age 9, medical degree at 21 - Dr. Yano is the youngest student to get an M.D. from UChicago http://goo.gl/qkqNh -- Disclaimer: I am an assistant professor of medicine and pediatrics at UChicago and have met Dr. Yano in our clinic.
The articles were selected from my Twitter and Google Reader streams. Please feel free to send suggestions for articles to clinicalcases@gmail.com and you will receive acknowledgement in the next edition of this publication.
Here are my suggestions for some of the top articles in medicine in June 2012:Cancer rates worldwide are expected to increase by 75% by 2030 http://goo.gl/Wu8i9
Zinc could be useful adjunct treatment in infants with probable serious bacterial infection - The Lancet http://goo.gl/Hgqs7
To screen or not to screen for prostate cancer? Fewer than 2% of Johns Hopkins doctors plan to follow the recommendations and stop ordering PSA screening - Lancet http://goo.gl/5Nkha
Dark chocolate could work as prevention therapy of cardiovascular disease - BMJ's exercise in wishful thinking: http://goo.gl/Om6kq
UV protection and sunscreens: What to tell patients - CCJM http://goo.gl/yhRH4 -- Related reading: How to avoid damaging ultraviolet light - CCJM launches "Patient Page" similar to JAMA http://bit.ly/MkL6Ae
NYTimes asks experts what they want from the future: "permanent sunblock that embeds in skin ~ Lasik eye surgery" ?! http://goo.gl/TnHZa -- Related: 32 Innovations Will Change Your Tomorrow - underwear with sensors tells how hard you’re working your quadriceps muscles http://goo.gl/EWRuX
Psoriasis: Evolving treatment for a complex disease - CCJM 2012 review, free full text http://goo.gl/Sc9Uy
Acute community-acquired bacterial meningitis in adults: CCJM 2012 review, free full text http://goo.gl/XKYQR
"Walmart clinics go live in the cloud": retail giant pushes healthcare providers to make diagnoses over the internet http://goo.gl/P51NW
A Single Inhalation of Laninamivir Works in Children With Influenza (study) http://goo.gl/BxgRs
Inhaled Hypertonic Saline (3%) mixed with albuterol reduces length of stay and admission rate for wheezing children http://goo.gl/g9cFH
College freshman at age 9, medical degree at 21 - Dr. Yano is the youngest student to get an M.D. from UChicago http://goo.gl/qkqNh -- Disclaimer: I am an assistant professor of medicine and pediatrics at UChicago and have met Dr. Yano in our clinic.
The articles were selected from my Twitter and Google Reader streams. Please feel free to send suggestions for articles to clinicalcases@gmail.com and you will receive acknowledgement in the next edition of this publication.
New treatment for dry eyes: "LipiFlow" uses heat and pressure to open blocked eyelid oil glands
To contact us Click HERE
The Meibomian glands (or tarsal glands) are sebaceous glands at the rim of the eyelids, responsible for the supply of meibum, an oily substance that prevents evaporation of the eye's tear film. They prevent tear spillage onto the cheek, trapping tears between the oiled edge and eyeball, and make the closed lids airtight. There are approximately 50 glands on the upper eyelids and 25 glands on the lower eyelids. The glands are named after Heinrich Meibom (1638–1700), a German physician (source: Wikipedia).
The LipiFlow Thermal Pulsation System uses heat and pressure to open blockages of the eyelid (Meibomian) glands. The treatment was approved by the FDA in 2011. Here is more information: http://lipiflow.com
Here is a Mayo Clinic video about the procedure:
The LipiFlow Thermal Pulsation System uses heat and pressure to open blockages of the eyelid (Meibomian) glands. The treatment was approved by the FDA in 2011. Here is more information: http://lipiflow.com
Here is a Mayo Clinic video about the procedure:
An App for Medical Emergencies - EmergencyLink - WSJ video
To contact us Click HERE
EmergencyLink is a free service that provides medical information and personal contacts to emergency responders - Mossberg for WSJ:
Here is the URL: http://www.emergencylink.com
The company explains how it can help if:
- You Are In An Accident. A first responder locates the EmergencyLink ID and calls EmergencyLink as instructed. EmergencyLink provides the first responder with your emergency medical information and contacts your “Emergency Contacts” as you have instructed.
- Your Child Is Missing. You can quickly create a a Missing Person report and forward it to the police. The police can immediately act on the information maximizing their chances of locating your child quickly and safely.
- Sharing Information with a Caregiver. You are able to electronically share all of the information the caregiver will need in case of an emergency. Whenever your child's profile is updated, everyone with whom you are sharing the information will be updated, no need to constantly update everyone.
- A Friend is in an Accident. If your friend is an EmergencyLink Member and is "sharing" their info with you, you can access their emergency medical information (allergies, medications, medical insurance) and forward them to the first responder.
- Co-Workers Are On A Project Away From Home. Each Member in the group agrees to share their emergency contact information with each other. If there is an emergency situation, the group has the information needed to reach each others emergency contacts.
EmergencyLink is a free 24-Hour Emergency Response Service that helps you store your important information in one location, share emergency information with family and friends and has a 24-Hour Emergency Response center to aid you in an emergency:
Here is the URL: http://www.emergencylink.com
The company explains how it can help if:
- You Are In An Accident. A first responder locates the EmergencyLink ID and calls EmergencyLink as instructed. EmergencyLink provides the first responder with your emergency medical information and contacts your “Emergency Contacts” as you have instructed.
- Your Child Is Missing. You can quickly create a a Missing Person report and forward it to the police. The police can immediately act on the information maximizing their chances of locating your child quickly and safely.
- Sharing Information with a Caregiver. You are able to electronically share all of the information the caregiver will need in case of an emergency. Whenever your child's profile is updated, everyone with whom you are sharing the information will be updated, no need to constantly update everyone.
- A Friend is in an Accident. If your friend is an EmergencyLink Member and is "sharing" their info with you, you can access their emergency medical information (allergies, medications, medical insurance) and forward them to the first responder.
- Co-Workers Are On A Project Away From Home. Each Member in the group agrees to share their emergency contact information with each other. If there is an emergency situation, the group has the information needed to reach each others emergency contacts.
EmergencyLink is a free 24-Hour Emergency Response Service that helps you store your important information in one location, share emergency information with family and friends and has a 24-Hour Emergency Response center to aid you in an emergency:
8 Temmuz 2012 Pazar
Polysensitization is more prevalent than monosensitization - will single allergen immunotherapy help?
To contact us Click HERE
 In patients seeking treatment for moderate-to-severe respiratory allergies, polysensitization is more prevalent (range, 50% to 80%) than monosensitization in both the United States and Europe.
In patients seeking treatment for moderate-to-severe respiratory allergies, polysensitization is more prevalent (range, 50% to 80%) than monosensitization in both the United States and Europe.
Europe vs. U.S. practices
In allergen immunotherapy there is debate as to whether:
1. polysensitized patients are best treated with many allergens simultaneously (chosen according to the sensitization profile, a predominantly North American approach)
2. a single allergen is the best approach (chosen according to the most clinically problematic allergy, a predominantly European approach)
In Europe most formulations are single-allergen extracts, whereas preparations in the United States contain an average of 8 different components.
The prevailing view in Europe is that a polysensitized patient is not necessarily polyallergic. The most troublesome allergy is then treated with a single-allergen preparation.
The predominant view in the United States is that there is an advantage in treating as many of the patient’s actual or potential sensitizations/allergies as possible. American allergists prefer to include all relevant allergens because of the concern over the significant time investment needed in SCIT, especially during the build-up phase. The standard US practice is to treat all relevant allergens.
What to do?
In patients with seasonal allergic rhinitis, subcutaneously and sublingually administered single-allergen preparations (grass pollen extracts) are clearly efficacious and safe.
Multiallergen immunotherapy faces formulation issues in a new era of registered and standardized allergen immunotherapies with numerous quality, efficacy, and safety constraints.
The US practice guidelines recommend that physicians treat with “relevant” allergens, although the interpretation of “relevant” can be problematic. For grass pollen allergens, trials show that polysensitized patients benefit just as much from single-allergen immunotherapy as monosensitized patients.
References:
Multiple-allergen and single-allergen immunotherapy strategies in polysensitized patients: Looking at the published evidence. JACI, 2012
Image source: OpenClipArt.org, public domain.
In patients seeking treatment for moderate-to-severe respiratory allergies, polysensitization is more prevalent (range, 50% to 80%) than monosensitization in both the United States and Europe.Europe vs. U.S. practices
In allergen immunotherapy there is debate as to whether:
1. polysensitized patients are best treated with many allergens simultaneously (chosen according to the sensitization profile, a predominantly North American approach)
2. a single allergen is the best approach (chosen according to the most clinically problematic allergy, a predominantly European approach)
In Europe most formulations are single-allergen extracts, whereas preparations in the United States contain an average of 8 different components.
The prevailing view in Europe is that a polysensitized patient is not necessarily polyallergic. The most troublesome allergy is then treated with a single-allergen preparation.
The predominant view in the United States is that there is an advantage in treating as many of the patient’s actual or potential sensitizations/allergies as possible. American allergists prefer to include all relevant allergens because of the concern over the significant time investment needed in SCIT, especially during the build-up phase. The standard US practice is to treat all relevant allergens.
What to do?
In patients with seasonal allergic rhinitis, subcutaneously and sublingually administered single-allergen preparations (grass pollen extracts) are clearly efficacious and safe.
Multiallergen immunotherapy faces formulation issues in a new era of registered and standardized allergen immunotherapies with numerous quality, efficacy, and safety constraints.
The US practice guidelines recommend that physicians treat with “relevant” allergens, although the interpretation of “relevant” can be problematic. For grass pollen allergens, trials show that polysensitized patients benefit just as much from single-allergen immunotherapy as monosensitized patients.
References:
Multiple-allergen and single-allergen immunotherapy strategies in polysensitized patients: Looking at the published evidence. JACI, 2012
Image source: OpenClipArt.org, public domain.
Drug Allergy Less Prevalent than Previously Assumed (study)
To contact us Click HERE
This 5-year analysis included 600 patients with suspected skin drug reactions, and 200 patients were invited for complete work-up with skin tests (prick/intracutaneous testing and scratch/patch, as indicated) and, if necessary, lymphocyte transformation tests (LTT).
140 patients underwent full work-up (75% female, 25% male). In 76% a drug was identified as the cause of the rash.
Among the skin drug reactions:
- 40% were caused by antibiotics
- 21% by anti-inflammatories
- 8% by contrast media
- 31% by other medications (oral antidiabetics, antimycotics, antipsychotics, antiepileptics and others)
The authors concluded that clinical assessment overestimated the role of drug allergies in cutaneous reactions.
Classification of adverse reactions to drugs, using the "SOAP III" mnemonic (click to enlarge the image):

References:
Is Drug Allergy Less Prevalent than Previously Assumed? Medscape, 2012.
140 patients underwent full work-up (75% female, 25% male). In 76% a drug was identified as the cause of the rash.
Among the skin drug reactions:
- 40% were caused by antibiotics
- 21% by anti-inflammatories
- 8% by contrast media
- 31% by other medications (oral antidiabetics, antimycotics, antipsychotics, antiepileptics and others)
The authors concluded that clinical assessment overestimated the role of drug allergies in cutaneous reactions.
Classification of adverse reactions to drugs, using the "SOAP III" mnemonic (click to enlarge the image):
References:
Is Drug Allergy Less Prevalent than Previously Assumed? Medscape, 2012.
Allergic rhinitis - top articles for June-July 2012
To contact us Click HERE
 Here are my suggestions for some of the top articles about allergic rhinitis in June-July 2012:
Here are my suggestions for some of the top articles about allergic rhinitis in June-July 2012:
Poor asthma control? – then look up the nose. The importance of co-morbid rhinitis in patients with asthma http://goo.gl/0nNZg
A new category of rhinitis based on localized atopy - local allergic rhinitis (LAR) http://goo.gl/Qlc5L and http://goo.gl/qaCdF
One type of Nonallergic rhinitis is classified as "Emotional" - JACI 2012, table 1 http://goo.gl/qaCdF
The burden of allergic rhinitis: persistent relief of symptoms remains a major unmet need http://goo.gl/jinfu
My Nasal Allergy Journal - free tools for patients by ACAAI http://goo.gl/Ynt81
Allergens in schools and homes: Mouse allergen levels in schools are substantial, followed by cat and dog http://goo.gl/hIUy1
Ragweed pollen collected along high-traffic roads shows a higher allergenicity http://goo.gl/HyTbp
Risk factors for chronic sinusitis in allergic rhinitis, from ENT perspective: infraorbital & frontal intersinus cells http://goo.gl/shthh
Lack of evidence to describe any dog breed as hypoallergenic: So-called hypoallergenic dogs had higher Can f 1 levels http://buff.ly/LAGGDx
Intranasal mometasone relieves itchy ear and palate, commonly reported with seasonal allergic rhinitis http://goo.gl/Fw6Jf
Is nasal saline irrigation all it is cracked up to be? Small clinical benefit, with minimal side effects http://goo.gl/J44b5
Analysis of mite allergic patients in a diverse territory by improved diagnostic tools: http://goo.gl/NaScp
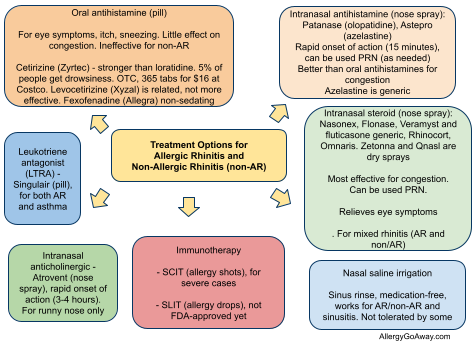
Treatment Options for Allergic Rhinitis and Non-Allergic Rhinitis (click to enlarge the image):
The articles were selected from my Twitter and Google Reader streams. Please feel free to send suggestions for articles to allergycases@gmail.com and you will receive acknowledgement in the next edition of this publication.
Image source: Illustration for "Aquiline or Roman Nose", Wikipedia, GNU Free Documentation License.
 Here are my suggestions for some of the top articles about allergic rhinitis in June-July 2012:
Here are my suggestions for some of the top articles about allergic rhinitis in June-July 2012:Poor asthma control? – then look up the nose. The importance of co-morbid rhinitis in patients with asthma http://goo.gl/0nNZg
A new category of rhinitis based on localized atopy - local allergic rhinitis (LAR) http://goo.gl/Qlc5L and http://goo.gl/qaCdF
One type of Nonallergic rhinitis is classified as "Emotional" - JACI 2012, table 1 http://goo.gl/qaCdF
The burden of allergic rhinitis: persistent relief of symptoms remains a major unmet need http://goo.gl/jinfu
My Nasal Allergy Journal - free tools for patients by ACAAI http://goo.gl/Ynt81
Allergens in schools and homes: Mouse allergen levels in schools are substantial, followed by cat and dog http://goo.gl/hIUy1
Ragweed pollen collected along high-traffic roads shows a higher allergenicity http://goo.gl/HyTbp
Risk factors for chronic sinusitis in allergic rhinitis, from ENT perspective: infraorbital & frontal intersinus cells http://goo.gl/shthh
Lack of evidence to describe any dog breed as hypoallergenic: So-called hypoallergenic dogs had higher Can f 1 levels http://buff.ly/LAGGDx
Intranasal mometasone relieves itchy ear and palate, commonly reported with seasonal allergic rhinitis http://goo.gl/Fw6Jf
Is nasal saline irrigation all it is cracked up to be? Small clinical benefit, with minimal side effects http://goo.gl/J44b5
Analysis of mite allergic patients in a diverse territory by improved diagnostic tools: http://goo.gl/NaScp
Treatment Options for Allergic Rhinitis and Non-Allergic Rhinitis (click to enlarge the image):
The articles were selected from my Twitter and Google Reader streams. Please feel free to send suggestions for articles to allergycases@gmail.com and you will receive acknowledgement in the next edition of this publication.
Image source: Illustration for "Aquiline or Roman Nose", Wikipedia, GNU Free Documentation License.
What is the typical laboratory evaluation of patients with common variable immunodeficiency (CVID)?
To contact us Click HERE
Here is the suggested Common Variable Immunodeficiency (CVID) workup, from AAAAI Ask the Expert:
Initial evaluation of CVID
- complete antibody workup for both several protein and anti-carbohydrate antibodies
- T and B and NK cells. Many centers do not routinely do mitogens and antigens, and routine HIV tests
- if liver tests are abnormal, one could do hepatitis tests
- CBD and CMP
- if there is a suspicion of lung disease, complete PFTs and a chest CT should be considered
- for suspicion of GI disease, malabsorption tests may be needed
Followup of CVID
While on IVIG or SCIG replacement, followup tests can included IgG level at 6 month intervals. If the patient only comes in only each year, then yearly IgG, CBC and CMP can be considered. Also, consider complete PFTs yearly. CT can be considered every 3 or 4 years, only if lung disease suspected or lung function is not normal.
Typical pattern of immunoglobulin levels (IgG, IgA, IgM) in humoral immunodeficiency. Click here to enlarge the table.

Primary immunodeficiency disorders (PIDD) (click to enlarge the image).
References:
Laboratory evaluation of patients with common variable immunodeficiency - AAAAI Ask the Expert, 2012.
Initial evaluation of CVID
- complete antibody workup for both several protein and anti-carbohydrate antibodies
- T and B and NK cells. Many centers do not routinely do mitogens and antigens, and routine HIV tests
- if liver tests are abnormal, one could do hepatitis tests
- CBD and CMP
- if there is a suspicion of lung disease, complete PFTs and a chest CT should be considered
- for suspicion of GI disease, malabsorption tests may be needed
Followup of CVID
While on IVIG or SCIG replacement, followup tests can included IgG level at 6 month intervals. If the patient only comes in only each year, then yearly IgG, CBC and CMP can be considered. Also, consider complete PFTs yearly. CT can be considered every 3 or 4 years, only if lung disease suspected or lung function is not normal.
Typical pattern of immunoglobulin levels (IgG, IgA, IgM) in humoral immunodeficiency. Click here to enlarge the table.
Primary immunodeficiency disorders (PIDD) (click to enlarge the image).
References:
Laboratory evaluation of patients with common variable immunodeficiency - AAAAI Ask the Expert, 2012.
Top Asthma Articles for June-July 2012
To contact us Click HERE
 Here are my suggestions for some of the top articles about asthma in June-July 2012:
Here are my suggestions for some of the top articles about asthma in June-July 2012:
The Chitin Connection: Treading the borderland between immunology, microbiology and severe asthma http://goo.gl/BcrpV via @AllergyNet
Free ACT questionnaire is superior to $5,000 FeNO device in determining asthma control in children http://goo.gl/OZdXR
Female gender is an independent risk factor for non-allergic asthma http://goo.gl/VqP1j
Allergic rhinitis is associated with poor asthma control in children with asthma - nasal corticosteroids may improve asthma control http://goo.gl/7vr5W
The public health benefits of air pollution control - free full text from JACI http://goo.gl/Yqw0K
Why does respiratory syncytial virus (RSV) appear to cause asthma? free full text from JACI http://goo.gl/2Tf1q
Omalizumab reduces on ED visits, hospitalizations, and corticosteroid use among patients with uncontrolled asthma http://buff.ly/LfiHHp
Stress can worsen asthma through mast cell activation (hypothesis) http://buff.ly/LfiwMa
No obvious benefit of salmeterol-fluticasone rather than fluticasone alone for steroid-naive children with multiple-trigger wheeze http://buff.ly/LAGggs
Another Reassuring Study on LABA-ICS Safety in Asthma - Medscape http://buff.ly/LAq4vN
Toward a definition of asthma phenotypes in childhood: early viral wheezers, multitrigger wheezers (MTWs), and nonatopic uncontrolled wheezers (NAUWs). Some children have “allergic bronchitis” rather than “asthma” http://goo.gl/16V3F
A new cell that could be causal in asthma: granulocyte population, termed type 2 myeloid (T2M) cells http://goo.gl/RGkjE
Advantages of montelukast in pediatric asthma: safety and oral administration (effectiveness, not so much) http://goo.gl/2CqdU
Children living on farms are protected against wheeze independently of atopy http://goo.gl/J689Z
The articles were selected from my Twitter stream @Allergy and Google Reader RSS subscriptions. Some of the top allergy accounts on Twitter contributed links. I appreciate the curation provided by @JuanCIvancevich @AllergyNet @IgECPD4 @DrAnneEllis @AACMaven @AllergieVoeding @allergistmommy @mrathkopf @wheezemd.
Please feel free to send suggestions for articles to allergycases@gmail.com and you will receive acknowledgement in the next edition of this publication.
Image source: Wikipedia, public domain.
Here are my suggestions for some of the top articles about asthma in June-July 2012:The Chitin Connection: Treading the borderland between immunology, microbiology and severe asthma http://goo.gl/BcrpV via @AllergyNet
Free ACT questionnaire is superior to $5,000 FeNO device in determining asthma control in children http://goo.gl/OZdXR
Female gender is an independent risk factor for non-allergic asthma http://goo.gl/VqP1j
Allergic rhinitis is associated with poor asthma control in children with asthma - nasal corticosteroids may improve asthma control http://goo.gl/7vr5W
The public health benefits of air pollution control - free full text from JACI http://goo.gl/Yqw0K
Why does respiratory syncytial virus (RSV) appear to cause asthma? free full text from JACI http://goo.gl/2Tf1q
Omalizumab reduces on ED visits, hospitalizations, and corticosteroid use among patients with uncontrolled asthma http://buff.ly/LfiHHp
Stress can worsen asthma through mast cell activation (hypothesis) http://buff.ly/LfiwMa
No obvious benefit of salmeterol-fluticasone rather than fluticasone alone for steroid-naive children with multiple-trigger wheeze http://buff.ly/LAGggs
Another Reassuring Study on LABA-ICS Safety in Asthma - Medscape http://buff.ly/LAq4vN
Toward a definition of asthma phenotypes in childhood: early viral wheezers, multitrigger wheezers (MTWs), and nonatopic uncontrolled wheezers (NAUWs). Some children have “allergic bronchitis” rather than “asthma” http://goo.gl/16V3F
A new cell that could be causal in asthma: granulocyte population, termed type 2 myeloid (T2M) cells http://goo.gl/RGkjE
Advantages of montelukast in pediatric asthma: safety and oral administration (effectiveness, not so much) http://goo.gl/2CqdU
Children living on farms are protected against wheeze independently of atopy http://goo.gl/J689Z
The articles were selected from my Twitter stream @Allergy and Google Reader RSS subscriptions. Some of the top allergy accounts on Twitter contributed links. I appreciate the curation provided by @JuanCIvancevich @AllergyNet @IgECPD4 @DrAnneEllis @AACMaven @AllergieVoeding @allergistmommy @mrathkopf @wheezemd.
Please feel free to send suggestions for articles to allergycases@gmail.com and you will receive acknowledgement in the next edition of this publication.
Image source: Wikipedia, public domain.
7 Temmuz 2012 Cumartesi
Acute low back pain: What to do? What works and what doesn't?
To contact us Click HERE
 Here is an excerpt from a recent review article in the official AFP journal American Family Physician:
Here is an excerpt from a recent review article in the official AFP journal American Family Physician:
Acute low back pain is one of the most common reasons for adults to see a physician. Most patients recover quickly with minimal treatment.
"Red flags"
Serious "red flags" include:
- significant trauma related to age (i.e., injury related to a fall from a height or motor vehicle crash in a young patient, or from a minor fall or heavy lifting in a patient with osteoporosis or possible osteoporosis)
- major or progressive motor or sensory deficit
- new-onset bowel or bladder incontinence or urinary retention
- loss of anal sphincter tone
- saddle anesthesia
- history of cancer metastatic to bone
- suspected spinal infection
Diagnosis
Without signs of serious pathology, imaging and laboratory testing often are not required.
Treatment
Patient education, nonsteroidal anti-inflammatory drugs (NSAIDs), acetaminophen, and muscle relaxants are beneficial.
Bed rest should be avoided, if possible.
Exercises directed by a physical therapist, such as the McKenzie method and spine stabilization exercises, may decrease recurrent pain.
Spinal manipulation and chiropractic techniques are no more effective than established medical treatments.
No substantial benefit has been shown with:
- oral steroids
- acupuncture
- massage
- traction
- lumbar supports
- regular exercise programs
References:
Diagnosis and treatment of acute low back pain. Casazza BA. Am Fam Physician. 2012 Feb 15;85(4):343-50.
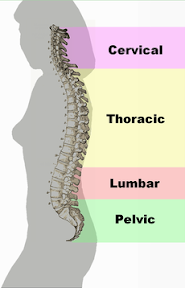
Image source: Different regions (curvatures) of the vertebral column, Wikipedia, public domain.
 Here is an excerpt from a recent review article in the official AFP journal American Family Physician:
Here is an excerpt from a recent review article in the official AFP journal American Family Physician:Acute low back pain is one of the most common reasons for adults to see a physician. Most patients recover quickly with minimal treatment.
"Red flags"
Serious "red flags" include:
- significant trauma related to age (i.e., injury related to a fall from a height or motor vehicle crash in a young patient, or from a minor fall or heavy lifting in a patient with osteoporosis or possible osteoporosis)
- major or progressive motor or sensory deficit
- new-onset bowel or bladder incontinence or urinary retention
- loss of anal sphincter tone
- saddle anesthesia
- history of cancer metastatic to bone
- suspected spinal infection
Diagnosis
Without signs of serious pathology, imaging and laboratory testing often are not required.
Treatment
Patient education, nonsteroidal anti-inflammatory drugs (NSAIDs), acetaminophen, and muscle relaxants are beneficial.
Bed rest should be avoided, if possible.
Exercises directed by a physical therapist, such as the McKenzie method and spine stabilization exercises, may decrease recurrent pain.
Spinal manipulation and chiropractic techniques are no more effective than established medical treatments.
No substantial benefit has been shown with:
- oral steroids
- acupuncture
- massage
- traction
- lumbar supports
- regular exercise programs
References:
Diagnosis and treatment of acute low back pain. Casazza BA. Am Fam Physician. 2012 Feb 15;85(4):343-50.
Image source: Different regions (curvatures) of the vertebral column, Wikipedia, public domain.
Genital ulcers - 2012 review from Am Fam Physician
To contact us Click HERE
Here is an excerpt from a review article in the official AAFP journal American Family Physician:
Causes of genital ulcers
Herpes simplex virus (HSV) infection and syphilis are the most common causes of genital ulcers in the U.S.
Other infectious causes include:
- chancroid
- lymphogranuloma venereum (LGV)
- granuloma inguinale (donovanosis)
- secondary bacterial infections
- fungi
Noninfectious etiologies of genital ulcers include:
- sexual trauma
- psoriasis
- Behçet syndrome
- fixed drug eruptions
CDC Streaming Health | This video, produced by Be Smart. Be Well., raises awareness of Sexually Transmitted Diseases (STDs): 1) What are they? 2) Why they matter? and, 3) What can I do about them? Footage courtesy of Be Smart. Be Well. http://www.besmartbewell.com, featuring CDC's Dr. John Douglas, Division of Sexually Transmitted Disease Prevention.
Diagnosis
The following tests should be considered in all patients:
- serologic tests for syphilis and darkfield microscopy or direct fluorescent antibody testing for Treponema pallidum
- culture or polymerase chain reaction test for herpes simplex virus (HSV)
- culture for Haemophilus ducreyi in settings with a high prevalence of chancroid
No pathogen is identified in up to 25% of patients with genital ulcers.
Treatment
The first episode of herpes simplex virus infection is usually treated with 7-10 days of oral acyclovir (5 days for recurrent episodes). Famciclovir and valacyclovir are alternative therapies.
One dose of intramuscular penicillin G benzathine is recommended to treat genital ulcers caused by primary syphilis.
Treatment options for chancroid include a single dose of intramuscular ceftriaxone or oral azithromycin, ciprofloxacin, or erythromycin.
Lymphogranuloma venereum and donovanosis are treated with 21 days of oral doxycycline.
Treatment of noninfectious causes of genital ulcers varies by etiology, of course. Topical wound care for ulcers caused by sexual trauma. Subcutaneous pegylated interferon alfa-2a is considered for ulcers caused by Behçet syndrome.
References:
Diagnosis and management of genital ulcers. Roett MA, Mayor MT, Uduhiri KA. Am Fam Physician. 2012 Feb 1;85(3):254-62.
Causes of genital ulcers
Herpes simplex virus (HSV) infection and syphilis are the most common causes of genital ulcers in the U.S.
Other infectious causes include:
- chancroid
- lymphogranuloma venereum (LGV)
- granuloma inguinale (donovanosis)
- secondary bacterial infections
- fungi
Noninfectious etiologies of genital ulcers include:
- sexual trauma
- psoriasis
- Behçet syndrome
- fixed drug eruptions
CDC Streaming Health | This video, produced by Be Smart. Be Well., raises awareness of Sexually Transmitted Diseases (STDs): 1) What are they? 2) Why they matter? and, 3) What can I do about them? Footage courtesy of Be Smart. Be Well. http://www.besmartbewell.com, featuring CDC's Dr. John Douglas, Division of Sexually Transmitted Disease Prevention.
Diagnosis
The following tests should be considered in all patients:
- serologic tests for syphilis and darkfield microscopy or direct fluorescent antibody testing for Treponema pallidum
- culture or polymerase chain reaction test for herpes simplex virus (HSV)
- culture for Haemophilus ducreyi in settings with a high prevalence of chancroid
No pathogen is identified in up to 25% of patients with genital ulcers.
Treatment
The first episode of herpes simplex virus infection is usually treated with 7-10 days of oral acyclovir (5 days for recurrent episodes). Famciclovir and valacyclovir are alternative therapies.
One dose of intramuscular penicillin G benzathine is recommended to treat genital ulcers caused by primary syphilis.
Treatment options for chancroid include a single dose of intramuscular ceftriaxone or oral azithromycin, ciprofloxacin, or erythromycin.
Lymphogranuloma venereum and donovanosis are treated with 21 days of oral doxycycline.
Treatment of noninfectious causes of genital ulcers varies by etiology, of course. Topical wound care for ulcers caused by sexual trauma. Subcutaneous pegylated interferon alfa-2a is considered for ulcers caused by Behçet syndrome.
References:
Diagnosis and management of genital ulcers. Roett MA, Mayor MT, Uduhiri KA. Am Fam Physician. 2012 Feb 1;85(3):254-62.
Healthcare social media #HCSM - top articles
To contact us Click HERE
 Here are my suggestions for some of the top articles related to healthcare social media (#HCSM) in the past 2 weeks:
Here are my suggestions for some of the top articles related to healthcare social media (#HCSM) in the past 2 weeks:
Facebook's user growth rate in the U.S. is slowing sharply http://goo.gl/wGO4c
Making social media work professionally in sensitive jobs – teaching, the police, healthcare http://goo.gl/ywfSP
A Brief Social Media Guide for Authors of Medical Resources http://goo.gl/6n17e
Phil Baumann: I hope that there is never ever going to be a “Facebook for Healthcare” http://goo.gl/hh3cI
Are hospitals into social media? A worldwide map: http://goo.gl/AAly2
Cleveland Clinic summit on Patient Experience shares presentation slides - a must-read for those interested in #HCSM http://goo.gl/EnMbK
Vote for 100 Most Influential People in Heathcare http://goo.gl/LXOhd - Not a single medical blogger apart from @Bob_Wachter made the list
10 Survey Tools for Bloggers http://goo.gl/8z21Y
Doctors use YouTube to build their personal brand by putting their expertise on video http://goo.gl/BQkGU
Millions of Healthcare Hashtags in the Symplur project - a vast database of information that can mined http://goo.gl/099ld
4 ways social media can improve your medical practice - AMA MedNews http://goo.gl/4b2RZ
2012 Physicians Survey reveals dissatisfaction and gloomy outlook - Orthopedic surgeon Howard J. Luks, shows the way forward http://goo.gl/eBzUA
The articles were selected from my Twitter and Google Reader streams. Please feel free to send suggestions for articles to clinicalcases@gmail.com and you will receive an acknowledgement in the next edition of this publication.
Facebook's user growth rate in the U.S. is slowing sharply http://goo.gl/wGO4c
Making social media work professionally in sensitive jobs – teaching, the police, healthcare http://goo.gl/ywfSP
A Brief Social Media Guide for Authors of Medical Resources http://goo.gl/6n17e
Phil Baumann: I hope that there is never ever going to be a “Facebook for Healthcare” http://goo.gl/hh3cI
Are hospitals into social media? A worldwide map: http://goo.gl/AAly2
Cleveland Clinic summit on Patient Experience shares presentation slides - a must-read for those interested in #HCSM http://goo.gl/EnMbK
Vote for 100 Most Influential People in Heathcare http://goo.gl/LXOhd - Not a single medical blogger apart from @Bob_Wachter made the list
10 Survey Tools for Bloggers http://goo.gl/8z21Y
Doctors use YouTube to build their personal brand by putting their expertise on video http://goo.gl/BQkGU
Millions of Healthcare Hashtags in the Symplur project - a vast database of information that can mined http://goo.gl/099ld
4 ways social media can improve your medical practice - AMA MedNews http://goo.gl/4b2RZ
2012 Physicians Survey reveals dissatisfaction and gloomy outlook - Orthopedic surgeon Howard J. Luks, shows the way forward http://goo.gl/eBzUA
The articles were selected from my Twitter and Google Reader streams. Please feel free to send suggestions for articles to clinicalcases@gmail.com and you will receive an acknowledgement in the next edition of this publication.
Top medicine articles for June 2012
To contact us Click HERE
Here are my suggestions for some of the top articles in medicine for June 2012:
Open access to research is inevitable, says Nature editor-in-chief http://goo.gl/N3OEU
Diagnosis, treatment, and management of echinococcosis | 2012 BMJ review http://goo.gl/r65Nd
How to be a cool headed clinician. Imperturbability is an essential characteristic for doctors, but how compatible is it with empathy? BMJ http://goo.gl/X7l5y
A doctor's guide to E/M coding - How to minimize lost revenue and likelihood of an audit - ModernMedicine http://goo.gl/RT6OC
Forgotten notebooks shed light on controversial discovery of streptomycin, the first antibiotic to cure TB http://goo.gl/1au0m
Apps for the Traveler With Medical Issues - NYTimes http://goo.gl/vFJzE
Statin Use Linked to Fatigue in Randomized Trial http://goo.gl/4xv0I and http://goo.gl/U2cMh
Thiazolidinedione use is associated with increased risk for diabetic macular edema http://goo.gl/1O0Tz
"Superbug" gonorrhea, becoming untreatable, accounts for 10% of STDs in Europe - doubling since last year http://goo.gl/y5aWr
Rapid Saliva Test for Laryngopharyngeal Reflux (LPR) http://goo.gl/LEsMO and http://goo.gl/GCean
Journal offers flat fee for ‘all you can publish’ Whereas PLoS ONE charges $1,350 per paper, PeerJ users pay $299 http://goo.gl/0kArd
Ipratropium linked to increased risk of stroke in COPD, especially with concomitant use of SABAs or theophylline http://goo.gl/CEr25
Chagas Disease is “The New HIV/AIDS of the Americas” claims the journal PLoS Neglected Tropical Diseases http://goo.gl/1P1qu
Cleveland Clinic summit on Patient Experience shares presentation slides - a must-read for those interested in #HCSM http://goo.gl/EnMbK
Doctors are using electronic records more - but liking them less - Washington Post http://buff.ly/Lpb8SY
Only 6.7% of office-based physicians routinely email with patients http://buff.ly/PPdusu
5 Key Benchmarks That Could Make or Break a Physician Practice http://buff.ly/LpbskH
90% of patients prefer web-based access to health information and education. 88% want to receive email reminders when it is time for preventive or follow-up care. 72% would like to use online services to book, change or cancel physician appointments. http://buff.ly/L0jjQS
The articles were selected from my Twitter and Google Reader streams. Please feel free to send suggestions for articles to clinicalcases@gmail.com and you will receive acknowledgement in the next edition of this publication.
Comments from Twitter:
Mike Cadogan @sandnsurf: Another great collection of the top #hcsm articles in medicine June 2012 via @DrVes litfl.com/LdO8X4
@DrVes: @sandnsurf @hjluks I'm glad you liked the summary http://casesblog.blogspot.com/2012/06/top-medicine-articles-for-june-2012.html - it's helpful to collect the article tweets for later reference.
Here are my suggestions for some of the top articles in medicine for June 2012:Open access to research is inevitable, says Nature editor-in-chief http://goo.gl/N3OEU
Diagnosis, treatment, and management of echinococcosis | 2012 BMJ review http://goo.gl/r65Nd
How to be a cool headed clinician. Imperturbability is an essential characteristic for doctors, but how compatible is it with empathy? BMJ http://goo.gl/X7l5y
A doctor's guide to E/M coding - How to minimize lost revenue and likelihood of an audit - ModernMedicine http://goo.gl/RT6OC
Forgotten notebooks shed light on controversial discovery of streptomycin, the first antibiotic to cure TB http://goo.gl/1au0m
Apps for the Traveler With Medical Issues - NYTimes http://goo.gl/vFJzE
Statin Use Linked to Fatigue in Randomized Trial http://goo.gl/4xv0I and http://goo.gl/U2cMh
Thiazolidinedione use is associated with increased risk for diabetic macular edema http://goo.gl/1O0Tz
"Superbug" gonorrhea, becoming untreatable, accounts for 10% of STDs in Europe - doubling since last year http://goo.gl/y5aWr
Rapid Saliva Test for Laryngopharyngeal Reflux (LPR) http://goo.gl/LEsMO and http://goo.gl/GCean
Journal offers flat fee for ‘all you can publish’ Whereas PLoS ONE charges $1,350 per paper, PeerJ users pay $299 http://goo.gl/0kArd
Ipratropium linked to increased risk of stroke in COPD, especially with concomitant use of SABAs or theophylline http://goo.gl/CEr25
Chagas Disease is “The New HIV/AIDS of the Americas” claims the journal PLoS Neglected Tropical Diseases http://goo.gl/1P1qu
Cleveland Clinic summit on Patient Experience shares presentation slides - a must-read for those interested in #HCSM http://goo.gl/EnMbK
Doctors are using electronic records more - but liking them less - Washington Post http://buff.ly/Lpb8SY
Only 6.7% of office-based physicians routinely email with patients http://buff.ly/PPdusu
5 Key Benchmarks That Could Make or Break a Physician Practice http://buff.ly/LpbskH
90% of patients prefer web-based access to health information and education. 88% want to receive email reminders when it is time for preventive or follow-up care. 72% would like to use online services to book, change or cancel physician appointments. http://buff.ly/L0jjQS
The articles were selected from my Twitter and Google Reader streams. Please feel free to send suggestions for articles to clinicalcases@gmail.com and you will receive acknowledgement in the next edition of this publication.
Comments from Twitter:
Mike Cadogan @sandnsurf: Another great collection of the top #hcsm articles in medicine June 2012 via @DrVes litfl.com/LdO8X4
@DrVes: @sandnsurf @hjluks I'm glad you liked the summary http://casesblog.blogspot.com/2012/06/top-medicine-articles-for-june-2012.html - it's helpful to collect the article tweets for later reference.
Top medicine articles for June-July 2012
To contact us Click HERE
Here are my suggestions for some of the top articles in medicine for June-July 2012:
Should You Put Sunscreen on Infants? It’s best not to use sunscreen on infants under age 6 months - FDA http://buff.ly/LxmJ0u
Guillain-Barre Syndrome - NEJM review http://buff.ly/LxmC55
Long-term use of low-dose azithromycin as an attractive adjunct treatment option for COPD http://buff.ly/LAoNVi
71% of doctors believe quality of healthcare will deteriorate over the next 5 years (19-page survey summary, PDF) http://goo.gl/Sl0wd
Americans' confidence in the U.S. medical system is around the historical average of 39% http://goo.gl/KoTqI
FDA Approves Diet Pill Belviq http://bit.ly/LCvE0o
What is So Good About Growing Old: mind gets sharper at a number of vitally important abilities http://goo.gl/6xI8M
A Lithium Battery in a Hotdog: the picture burns itself into mind - keep out of reach of small children http://buff.ly/LSmPBS
People who remember being pushed or slapped as children more likely to have depression or anxiety later in life http://goo.gl/oTt7p
Physical Punishment Has Long-Lasting Consequences on Children's Mental Health (study) http://buff.ly/LKGrl6
GSK once-daily lung drug LAMA/LABA (umeclidinium/vilanterol) showed positive results in COPD http://goo.gl/s1o0P
1 in 5 Nurses is Depressed - 18% of hospital-employed nurses have depression; twice the rate of the general public http://goo.gl/aioSn
The Medication Generation: Many young people today have now spent most of their lives on antidepressants - WSJ http://on.wsj.com/LLDuVE
Publishing a medical journal is a very profitable activity, says former BMJ Editor-in-Chief and provides examples http://goo.gl/QeaKS
Health Care Mandate Puts a "Cranky Uncle" in Every Exam Room - NYTimes http://goo.gl/v0PpH
The articles were selected from my Twitter and Google Reader streams. Please feel free to send suggestions for articles to clinicalcases@gmail.com and you will receive acknowledgement in the next edition of this publication.
Here are my suggestions for some of the top articles in medicine for June-July 2012:Should You Put Sunscreen on Infants? It’s best not to use sunscreen on infants under age 6 months - FDA http://buff.ly/LxmJ0u
Guillain-Barre Syndrome - NEJM review http://buff.ly/LxmC55
Long-term use of low-dose azithromycin as an attractive adjunct treatment option for COPD http://buff.ly/LAoNVi
71% of doctors believe quality of healthcare will deteriorate over the next 5 years (19-page survey summary, PDF) http://goo.gl/Sl0wd
Americans' confidence in the U.S. medical system is around the historical average of 39% http://goo.gl/KoTqI
FDA Approves Diet Pill Belviq http://bit.ly/LCvE0o
What is So Good About Growing Old: mind gets sharper at a number of vitally important abilities http://goo.gl/6xI8M
A Lithium Battery in a Hotdog: the picture burns itself into mind - keep out of reach of small children http://buff.ly/LSmPBS
People who remember being pushed or slapped as children more likely to have depression or anxiety later in life http://goo.gl/oTt7p
Physical Punishment Has Long-Lasting Consequences on Children's Mental Health (study) http://buff.ly/LKGrl6
GSK once-daily lung drug LAMA/LABA (umeclidinium/vilanterol) showed positive results in COPD http://goo.gl/s1o0P
1 in 5 Nurses is Depressed - 18% of hospital-employed nurses have depression; twice the rate of the general public http://goo.gl/aioSn
The Medication Generation: Many young people today have now spent most of their lives on antidepressants - WSJ http://on.wsj.com/LLDuVE
Publishing a medical journal is a very profitable activity, says former BMJ Editor-in-Chief and provides examples http://goo.gl/QeaKS
Health Care Mandate Puts a "Cranky Uncle" in Every Exam Room - NYTimes http://goo.gl/v0PpH
The articles were selected from my Twitter and Google Reader streams. Please feel free to send suggestions for articles to clinicalcases@gmail.com and you will receive acknowledgement in the next edition of this publication.
5 Temmuz 2012 Perşembe
Drowning Prevention Guidelines
To contact us Click HERE
Here is a video from the Cleveland Clinic:
Key risk factors for drowning are:
- male sex
- age of less than 14 years
- alcohol use
- low income
- poor education
- rural residency
- aquatic exposure
- risky behavior
- lack of supervision
For people with epilepsy, the risk of drowning is 15 to 19 times as high as the risk for those who do not have epilepsy.
For every person who dies from drowning, another four persons receive care in the emergency department for nonfatal drowning.
Drowning Doesn’t Look Like Drowning
- Except in rare circumstances, drowning people are physiologically unable to call out for help. The respiratory system was designed for breathing. Speech is the secondary or overlaid function. Breathing must be fulfilled, before speech occurs.
- Drowning people’s mouths alternately sink below and reappear above the surface of the water.
- The mouths of drowning people are not above the surface of the water long enough for them to exhale, inhale, and call out for help. When the drowning people’s mouths are above the surface, they exhale and inhale quickly as their mouths start to sink below the surface of the water.
- Drowning people cannot wave for help. Nature instinctively forces them to extend their arms laterally and press down on the water’s surface. Pressing down on the surface of the water, permits drowning people to leverage their bodies so they can lift their mouths out of the water to breathe.
- Throughout the Instinctive Drowning Response, drowning people cannot voluntarily control their arm movements. Physiologically, drowning people who are struggling on the surface of the water cannot stop drowning and perform voluntary movements such as waving for help, moving toward a rescuer, or reaching out for a piece of rescue equipment.
- From beginning to end of the Instinctive Drowning Response people’s bodies remain upright in the water, with no evidence of a supporting kick. Unless rescued by a trained lifeguard, these drowning people can only struggle on the surface of the water from 20 to 60 seconds before submersion occurs.
References:
Drowning Doesn’t Look Like Drowning. Mario Vittone.On Scene Magazine: Fall 2006 (page 14)
Drowning - free NEJM review, 2012 http://goo.gl/xSqLu
Key risk factors for drowning are:
- male sex
- age of less than 14 years
- alcohol use
- low income
- poor education
- rural residency
- aquatic exposure
- risky behavior
- lack of supervision
For people with epilepsy, the risk of drowning is 15 to 19 times as high as the risk for those who do not have epilepsy.
For every person who dies from drowning, another four persons receive care in the emergency department for nonfatal drowning.
Drowning Doesn’t Look Like Drowning
- Except in rare circumstances, drowning people are physiologically unable to call out for help. The respiratory system was designed for breathing. Speech is the secondary or overlaid function. Breathing must be fulfilled, before speech occurs.
- Drowning people’s mouths alternately sink below and reappear above the surface of the water.
- The mouths of drowning people are not above the surface of the water long enough for them to exhale, inhale, and call out for help. When the drowning people’s mouths are above the surface, they exhale and inhale quickly as their mouths start to sink below the surface of the water.
- Drowning people cannot wave for help. Nature instinctively forces them to extend their arms laterally and press down on the water’s surface. Pressing down on the surface of the water, permits drowning people to leverage their bodies so they can lift their mouths out of the water to breathe.
- Throughout the Instinctive Drowning Response, drowning people cannot voluntarily control their arm movements. Physiologically, drowning people who are struggling on the surface of the water cannot stop drowning and perform voluntary movements such as waving for help, moving toward a rescuer, or reaching out for a piece of rescue equipment.
- From beginning to end of the Instinctive Drowning Response people’s bodies remain upright in the water, with no evidence of a supporting kick. Unless rescued by a trained lifeguard, these drowning people can only struggle on the surface of the water from 20 to 60 seconds before submersion occurs.
References:
Drowning Doesn’t Look Like Drowning. Mario Vittone.On Scene Magazine: Fall 2006 (page 14)
Drowning - free NEJM review, 2012 http://goo.gl/xSqLu
Father's Day and Every Day - Take Care of Your Other Half
To contact us Click HERE

I usually write about infertility and miscarriage from a woman's point of view. But in honor of Father's Day, there's another important piece of the puzzle and that is how your husband and your relationship is fairing through infertility. I recall when my husband and I were going through fertility treatments. I was on so many different fertility drugs and hormone shots that I was pretty much a raving lunatic. What do you expect when you are pumping yourself up with all those chemicals? My husband used to think PMS was bad...
Even after our failed IVF's when we decided just to try naturally, it was a rollercoaster ride every month. It would start around the time of ovulation where intercourse was mandatory (UGGGGHHH) and it would end with the anger and tears when either the pregnancy test was negative or I got my period. I found a good article about preserving your relationship while struggling with infertility:
Keeping It Together During Infertility
Stay the course. Take care of each other. When that test finally comes out positive, you will know that it was all worth it. My husband and I also had to deal with recurrent miscarriage. But, even through it all, I just knew deep down that I would succeed (and that's probably why I did). When all is said and done, the rollercoaster ride won't seem so crazy, it becomes a distant memory. Let the hard times strengthen your relationship. When you celebrate Father's Day for real, your child/children will truly appreciate parents that 'kept it together'.
I usually write about infertility and miscarriage from a woman's point of view. But in honor of Father's Day, there's another important piece of the puzzle and that is how your husband and your relationship is fairing through infertility. I recall when my husband and I were going through fertility treatments. I was on so many different fertility drugs and hormone shots that I was pretty much a raving lunatic. What do you expect when you are pumping yourself up with all those chemicals? My husband used to think PMS was bad...
Even after our failed IVF's when we decided just to try naturally, it was a rollercoaster ride every month. It would start around the time of ovulation where intercourse was mandatory (UGGGGHHH) and it would end with the anger and tears when either the pregnancy test was negative or I got my period. I found a good article about preserving your relationship while struggling with infertility:
Keeping It Together During Infertility
Stay the course. Take care of each other. When that test finally comes out positive, you will know that it was all worth it. My husband and I also had to deal with recurrent miscarriage. But, even through it all, I just knew deep down that I would succeed (and that's probably why I did). When all is said and done, the rollercoaster ride won't seem so crazy, it becomes a distant memory. Let the hard times strengthen your relationship. When you celebrate Father's Day for real, your child/children will truly appreciate parents that 'kept it together'.
Flaxseeds For Men's Fertiliy
To contact us Click HERE

Overcome Male Infertility - How to Treat Infertility With Flaxseed
Overcome Male Infertility - How to Treat Infertility With Flaxseed
Guest Post By Kyle J Norton
As we mentioned in previous articles, infertility is defined as inability of a couple to conceive after 12 months of unprotected sexual intercourse. It effects over 5 millions couple alone in the U. S. and many times more in the world. Because of unawareness of treatments, only 10% seeks help from professional specialist.We have spent most of the time in this series discussing the conventional and Chinese medicine in treating fertility. I believe, it is the best time to change the subject by discussing how to treat male infertility with flaxseed oil.
I. Definition
Flax, also known Linum usitatissimum, is a member of the genus Linum. Belonging to the family Linaceae, it's seed has been used in traditional medicine in treating heart diseases caused by high levels of cholesterol.
II. How flaxseed oil effects male fertility
1. Essential fatty acid
Flaxseed oil contains high levels of essential fatty acid Omega 3 and 6, it not only help to eliminate the trans fat and saturate fat through liver waste elimination, but also helps to increasing blood flow to the reproductive organs resulting in increasing the production of sperm count and sperm quality.
2. Lignan
flaxseed contains high amount of ligan, it is proven in helping to strengthen not only the immune system in fighting against irregular cells growth, but also improve it's function in protecting the body own tissues, including sperm.
3. Lecithin
Lecithin is a fat like substance (phospholipid) found in flaxseed not only helps to inhibit the levels of bad cholesterol, but also is a key building block of cell membranes resulting in protecting protects cells from oxidation in the surrounding the brain, thus lessening the risk of nervous tension, hormone imbalance and low libido.
4. Fiber
Flax seeds contain high amount of fiber which is vital in helping liver in regulating spleen in insulin production, resulting in decreasing the risk of blood stagnation and qi imbalance in spleen, leading to normalizing the production of testosterone and increasing the chance of good quality sperm production.
5. Alpha linolenic acid
It also contains high levels of alpha linolenic acid which is vital for a healthy prostate gland, resulting in increasing the kidney function in regulating sperm production as well as strong ejaculation.
III. Side effects
1. Intestinal blockage, if it is taken in large amounts. Please remember to drink a lot of liquids to avoid this to happen.
2. Because of it' high concentration of fiber, it may reduce the effectiveness of some oral medicine.
For the best pregnancy self help program review, please visit http://bestfertility.blogspot.com/.
For series of Infertility Articles, please visit http://fertility-infertility.blogspot.com/.
All rights reserved. Any reproducing of this article must have the author name and all the links intact.
"Let You Be With Your Health, Let Your Health Be With You" -Kyle J. Norton
I have been studying natural remedies for disease prevention for over 20 years and working as a financial consultant since 1990. Master degree in Mathematics, teaching and tutoring math at colleges and universities before joining insurance industries. Part time Health, Insurance and Entertainment Article Writer.
Article Source: http://EzineArticles.com/?expert=Kyle_J_Norton
http://EzineArticles.com/?Overcome-Male-Infertility---How-to-Treat-Infertility-With-Flaxseed&id=2765481

Overcome Male Infertility - How to Treat Infertility With Flaxseed
Guest Post By Kyle J Norton
As we mentioned in previous articles, infertility is defined as inability of a couple to conceive after 12 months of unprotected sexual intercourse. It effects over 5 millions couple alone in the U. S. and many times more in the world. Because of unawareness of treatments, only 10% seeks help from professional specialist.We have spent most of the time in this series discussing the conventional and Chinese medicine in treating fertility. I believe, it is the best time to change the subject by discussing how to treat male infertility with flaxseed oil.
I. Definition
Flax, also known Linum usitatissimum, is a member of the genus Linum. Belonging to the family Linaceae, it's seed has been used in traditional medicine in treating heart diseases caused by high levels of cholesterol.
II. How flaxseed oil effects male fertility
1. Essential fatty acid
Flaxseed oil contains high levels of essential fatty acid Omega 3 and 6, it not only help to eliminate the trans fat and saturate fat through liver waste elimination, but also helps to increasing blood flow to the reproductive organs resulting in increasing the production of sperm count and sperm quality.
2. Lignan
flaxseed contains high amount of ligan, it is proven in helping to strengthen not only the immune system in fighting against irregular cells growth, but also improve it's function in protecting the body own tissues, including sperm.
3. Lecithin
Lecithin is a fat like substance (phospholipid) found in flaxseed not only helps to inhibit the levels of bad cholesterol, but also is a key building block of cell membranes resulting in protecting protects cells from oxidation in the surrounding the brain, thus lessening the risk of nervous tension, hormone imbalance and low libido.
4. Fiber
Flax seeds contain high amount of fiber which is vital in helping liver in regulating spleen in insulin production, resulting in decreasing the risk of blood stagnation and qi imbalance in spleen, leading to normalizing the production of testosterone and increasing the chance of good quality sperm production.
5. Alpha linolenic acid
It also contains high levels of alpha linolenic acid which is vital for a healthy prostate gland, resulting in increasing the kidney function in regulating sperm production as well as strong ejaculation.
III. Side effects
1. Intestinal blockage, if it is taken in large amounts. Please remember to drink a lot of liquids to avoid this to happen.
2. Because of it' high concentration of fiber, it may reduce the effectiveness of some oral medicine.
For the best pregnancy self help program review, please visit http://bestfertility.blogspot.com/.
For series of Infertility Articles, please visit http://fertility-infertility.blogspot.com/.
All rights reserved. Any reproducing of this article must have the author name and all the links intact.
"Let You Be With Your Health, Let Your Health Be With You" -Kyle J. Norton
I have been studying natural remedies for disease prevention for over 20 years and working as a financial consultant since 1990. Master degree in Mathematics, teaching and tutoring math at colleges and universities before joining insurance industries. Part time Health, Insurance and Entertainment Article Writer.
Article Source: http://EzineArticles.com/?expert=Kyle_J_Norton
http://EzineArticles.com/?Overcome-Male-Infertility---How-to-Treat-Infertility-With-Flaxseed&id=2765481
Herbs Found to Be More Affective Than Traditional Fertility Treatment In Some Women
To contact us Click HERE

I did not take a lot of herbs when I was trying to conceive, however, I do know a number of women who did and succeeded in becoming pregnant. This interesting article talks about how one study found that herbal treatment may have higher success rates than tradition fertility treatments. Read more
www.naturalnews.com
From the article:
Study methodology
The study examined abstracts in English of studies investigating infertility, menstrual health and TCM. Researchers then did meta-analyses of (non)randomised controlled trials (RCTs) or cohort studies and compared clinical pregnancy rates achieved with Chinese herbal medicine versus Western medicine drug treatment (IVF). In addition, they collected common TCM pattern diagnosis in infertility in relation to the quality of the menstrual cycle and associated symptoms. Eight RCTs, 13 cohort studies, three case series and six case studies involving a total of 1851 women with infertility were included in the systematic review.
Results
The results showed a 3.5 greater likelihood of achieving a pregnancy with Chinese herbal medicine therapy over a four-month period compared with Western medicine drug therapy alone. Average pregnancy rates were 60 ± 12.5% (60%) for Chinese herbal medicine compared with 32 ± 10% (32%) using Western medicine drug therapy. Meta-analysis of selected cohort studies showed a mean clinical pregnancy rate of 50 percent using TCM compared with 30 percent for IVF.

I did not take a lot of herbs when I was trying to conceive, however, I do know a number of women who did and succeeded in becoming pregnant. This interesting article talks about how one study found that herbal treatment may have higher success rates than tradition fertility treatments. Read more
www.naturalnews.com
From the article:
Study methodology
The study examined abstracts in English of studies investigating infertility, menstrual health and TCM. Researchers then did meta-analyses of (non)randomised controlled trials (RCTs) or cohort studies and compared clinical pregnancy rates achieved with Chinese herbal medicine versus Western medicine drug treatment (IVF). In addition, they collected common TCM pattern diagnosis in infertility in relation to the quality of the menstrual cycle and associated symptoms. Eight RCTs, 13 cohort studies, three case series and six case studies involving a total of 1851 women with infertility were included in the systematic review.
Results
The results showed a 3.5 greater likelihood of achieving a pregnancy with Chinese herbal medicine therapy over a four-month period compared with Western medicine drug therapy alone. Average pregnancy rates were 60 ± 12.5% (60%) for Chinese herbal medicine compared with 32 ± 10% (32%) using Western medicine drug therapy. Meta-analysis of selected cohort studies showed a mean clinical pregnancy rate of 50 percent using TCM compared with 30 percent for IVF.
Trying To Get Pregnant: There's No Fireworks
To contact us Click HERE

Remember those old re-runs of a program called "Love American Style" (or in my case you saw them the first time around)? Fireworks represented the love and infatuation associated with your relationship and/or marriage. Well, no matter how good your relationship is, when you're trying to conceive, every aspect of your life revolves around ovulation. Intercourse can become a total chore and no, there are absolutely no fireworks. I remember a few years on independence day, I was ovulating and we could hear our neighbors shooting off firecrakers--there we were trying to "get the job done". UGGGGHHHH...not pleasant memories at all.
Independence day is another one of those family oriented holidays. All you see around you are families packing up the car to go watch fireworks displays, kid-oriented events, BBQ's etc. It's another holiday where you stick out like a sore thumb. I recall going to a function with my husband's sister and their kids. We met a few of their friends and then the bomb dropped. One of their friends (who was there with his four kids) says to me..."I'll bet you guys have a bunch of kids right?" I was so taken off guard...he immediately sensed me squirming as I said sheepishly..."Uh no, we don't have any". End of conversation.
After that, we decided to have our own way of enjoying the holiday. We stayed away from BBQ's and had a nice dinner out. Hey, whatever works. I'm not saying you shouldn't join in (because we did that too), but you should do whatever helps you deal with the situation at the time.
So, whatever you do this holiday, please enjoy it safely and don't be afraid to go out and have some fun - even if it's not in the traditional way.
Remember those old re-runs of a program called "Love American Style" (or in my case you saw them the first time around)? Fireworks represented the love and infatuation associated with your relationship and/or marriage. Well, no matter how good your relationship is, when you're trying to conceive, every aspect of your life revolves around ovulation. Intercourse can become a total chore and no, there are absolutely no fireworks. I remember a few years on independence day, I was ovulating and we could hear our neighbors shooting off firecrakers--there we were trying to "get the job done". UGGGGHHHH...not pleasant memories at all.
Independence day is another one of those family oriented holidays. All you see around you are families packing up the car to go watch fireworks displays, kid-oriented events, BBQ's etc. It's another holiday where you stick out like a sore thumb. I recall going to a function with my husband's sister and their kids. We met a few of their friends and then the bomb dropped. One of their friends (who was there with his four kids) says to me..."I'll bet you guys have a bunch of kids right?" I was so taken off guard...he immediately sensed me squirming as I said sheepishly..."Uh no, we don't have any". End of conversation.
After that, we decided to have our own way of enjoying the holiday. We stayed away from BBQ's and had a nice dinner out. Hey, whatever works. I'm not saying you shouldn't join in (because we did that too), but you should do whatever helps you deal with the situation at the time.
So, whatever you do this holiday, please enjoy it safely and don't be afraid to go out and have some fun - even if it's not in the traditional way.
4 Temmuz 2012 Çarşamba
Onward
To contact us Click HERE
In upcoming posts, I plan to pursue two main themes. The first is a more comprehensive exploration of what determines eating behavior in humans, the neurobiology behind it, and the real world implications of this research. The reward and palatability value of food are major factors, but there are others, and I've spent enough time focusing on them for the time being. Also, the discussions revolving around food reward seem to be devolving into something that resembles team sports, and I've had my fill.
The second topic I'm going to touch on is human evolutionary history, including amazing recent insights from the field of human genetics. These findings have implications for the nutrition and health of modern humans.
I look forward to exploring these topics, and others, with all of you in the coming months.
The second topic I'm going to touch on is human evolutionary history, including amazing recent insights from the field of human genetics. These findings have implications for the nutrition and health of modern humans.
I look forward to exploring these topics, and others, with all of you in the coming months.
The Eocene Diet
To contact us Click HERE
65 million years ago, a massive asteroid slammed into the Yucatan peninsula, creating a giant dust cloud that contributed to the extinction of terrestrial dinosaurs. In the resulting re-adjustment of global ecosystems, a new plant tissue evolved, which paved the way for the eventual appearance of humans: fruit. Fruit represents a finely crafted symbiosis between plants and animals, in which the plant provides a nourishing morsel, and the animal disperses the plant's seeds inside a packet of rich fertilizer.
Fruit was such a powerful selective pressure that mammals quickly evolved to exploit it more effectively, developing adaptations for life in the forest canopy. One result of this was the rapid emergence of primates, carrying physical, digestive and metabolic adaptations for the acquisition and consumption of fruit and leaves. Primates also continued eating insects, a vestige of our early mammalian heritage.
The Eocene epoch began 55.8 million years ago, just after the emergence of primates. For most of the time between the beginning of the Eocene and today, our ancestors ate the archetypal primate diet of fruit, leaves and insects, just as most primates do today.
In contrast, the Paleolithic era, marked by the development of stone tools and a dietary shift toward meat and cooked starches, began only 2.6 million years ago. The Paleolithic era represents only 5 percent of the time that shaped our primate genome-- 95 percent of primate evolutionary history occurred prior to the Paleolithic. The Neolithic period, since humans domesticated plants roughly 10,000 years ago, accounts for only 0.02 percent.
Therefore, we are not well adapted to eating grains, legumes and dairy, and we aren't well adapted to eating meat and starch either. Our true, deepest evolutionary adaptations are to the foods that sustained our primate ancestors for the tens of millions of years prior to the Paleolithic. That's why I designed the Eocene Diet (TM).
The Eocene Diet is easy. You simply eat these three foods:

Fruit and leaves are easy to find, but what about insects? With a little practice, you'll see that they're easy to find too, often for free. Here are some tips:

She looks pleased.
The Eocene Diet is so effective for weight loss and general health that I've come up with this slogan for it:
Fruit was such a powerful selective pressure that mammals quickly evolved to exploit it more effectively, developing adaptations for life in the forest canopy. One result of this was the rapid emergence of primates, carrying physical, digestive and metabolic adaptations for the acquisition and consumption of fruit and leaves. Primates also continued eating insects, a vestige of our early mammalian heritage.
The Eocene epoch began 55.8 million years ago, just after the emergence of primates. For most of the time between the beginning of the Eocene and today, our ancestors ate the archetypal primate diet of fruit, leaves and insects, just as most primates do today.
In contrast, the Paleolithic era, marked by the development of stone tools and a dietary shift toward meat and cooked starches, began only 2.6 million years ago. The Paleolithic era represents only 5 percent of the time that shaped our primate genome-- 95 percent of primate evolutionary history occurred prior to the Paleolithic. The Neolithic period, since humans domesticated plants roughly 10,000 years ago, accounts for only 0.02 percent.
Therefore, we are not well adapted to eating grains, legumes and dairy, and we aren't well adapted to eating meat and starch either. Our true, deepest evolutionary adaptations are to the foods that sustained our primate ancestors for the tens of millions of years prior to the Paleolithic. That's why I designed the Eocene Diet (TM).
The Eocene Diet is easy. You simply eat these three foods:
- Raw fruit
- Raw leaves (no dressing!)
- Live insects
Fruit and leaves are easy to find, but what about insects? With a little practice, you'll see that they're easy to find too, often for free. Here are some tips:
- Pet stores. They usually sell crickets and mealworms.
- Look under rotting logs.
- Find a long, flexible stem and stick it into a termite mound. Termites will grab onto it and you can eat them off the stem.
She looks pleased.
The Eocene Diet is so effective for weight loss and general health that I've come up with this slogan for it:
"You WILL lose weight on the Eocene Diet (TM). Even if you don't want to. I guarantee it!"April Fools!
Eocene Diet Follow-up
To contact us Click HERE
Now that WHS readers around the globe have adopted the Eocene Diet and are losing weight at an alarming rate, it's time to explain the post a little more. First, credit where credit is due: Melissa McEwen made a similar argument in her 2011 AHS talk, where she rolled out the "Cambrian Explosion Diet", which beats the Eocene Diet by about 470 million years. It was probably in the back of my head somewhere when I came up with the idea.
April Fools day is good for a laugh, but humor often has a grain of truth in it. In this case, the post was a jumping off point for discussing human evolution and what it has to say about the "optimal" human diet, if such a thing exists. Here's a preview: evolution is a continuous process that has shaped our ancestors' genomes for every generation since the beginning of life. It didn't end with the Paleolithic, in fact it accelerated, and most of us today carry meaningful adaptations to the Neolithic diet and lifestyle.
Modern genetics has revealed that we are all genetic patchwork quilts, our genomes shaped by several different environments, and perfectly adapted to none. We're caught in the middle of an evolutionary transition, partially adapted to Neolithic life but not quite there yet, and no longer quite adapted to the life of a hunter-gatherer either.
I'll delve into these topics further in upcoming posts, and introduce Ötzi, the Tyrolean ice man, who will be our guide.
April Fools day is good for a laugh, but humor often has a grain of truth in it. In this case, the post was a jumping off point for discussing human evolution and what it has to say about the "optimal" human diet, if such a thing exists. Here's a preview: evolution is a continuous process that has shaped our ancestors' genomes for every generation since the beginning of life. It didn't end with the Paleolithic, in fact it accelerated, and most of us today carry meaningful adaptations to the Neolithic diet and lifestyle.
Modern genetics has revealed that we are all genetic patchwork quilts, our genomes shaped by several different environments, and perfectly adapted to none. We're caught in the middle of an evolutionary transition, partially adapted to Neolithic life but not quite there yet, and no longer quite adapted to the life of a hunter-gatherer either.
I'll delve into these topics further in upcoming posts, and introduce Ötzi, the Tyrolean ice man, who will be our guide.
New Study: Is a Calorie a Calorie?
To contact us Click HERE
A new study in JAMA led by Dr. Cara B. Ebbeling and colleagues purports to challenge the idea that all calories are equally fattening (1). Let's have a look. When thinking about the role of calorie intake in body fatness, there are basically three camps:
1. Calories don’t matter at all, only diet composition matters.
2. Calories are the only thing that matters, and diet composition is irrelevant.
3. Calories matter, but diet composition may also play a role.
The first one is an odd position that is not very well populated. The second one has a lot of adherents in the research world, and there’s enough evidence to make a good case for it. It’s represented by the phrase ‘a calorie is a calorie’, i.e. all calories are equally fattening. #1 and #2 are both extreme positions, and as such they get a lot of attention. But the third group, although less vocal, may be closest to the truth.
A Little Background on Food Intake, Diet Composition and Energy Expenditure
The energy content of the human body is determined by the amount of energy coming in, minus the energy exiting—simple on paper. Since body fat is by far the main energy storage site in the body, it follows that the balance between energy intake and energy expenditure determines fat mass, and this has been experimentally confirmed many times. But here’s the catch—energy expenditure is not always constant. For example, we know that it increases as a person gains weight, and decreases when a person loses weight (2). The decrease in energy expenditure with weight loss is caused by two things, 1) a smaller body requires fewer calories for maintenance, 2) a decrease in leptin, which decreases the metabolic rate by acting in the brain (3).
Some people have suggested that the type of food we eat, not just the amount, influences energy expenditure, and in particular that this is related to the diet's carbohydrate content. In people who are not trying to lose weight (4, 5), or who are being overfed (6, 7), the carbohydrate:fat ratio in the diet has little or no detectable impact on energy expenditure, and if anything it favors carbohydrate, but could this be different during fat loss in people who start off overweight? This idea has been called the ‘metabolic advantage’, most notably attributed to the low-carbohydrate diet. The idea here is that you can lose fat eating the same number of calories if carbohydrate is kept low.
I’ve never really weighed in on this because it’s a topic of heated debate, and in any case it’s a fairly academic question. Why is it academic? Because previous weight loss studies have shown that if a metabolic advantage exists at all, it’s quite small, because the effect is undetectable in most studies (8, 9, 10). People who are not associated with the low-carbohydrate community tend to conclude that there's no metabolic advantage when they review the literature (11), although I haven't reviewed it closely myself. It’s clear that where fat loss is concerned, calorie intake is much more important than the amount of fat or carbohydrate in the diet. What previous studies have suggested is that low-carbohydrate diets suppress appetite — often resulting in lower calorie intake (12, 13). The reason for this remains a topic of speculation.
That being said, I’m actually quite open to the idea that food quality in addition to quantity can influence body fatness, and I would encourage people to think outside the macronutrient box: there are probably many different dietary factors that can have such an effect. Although this idea hasn’t received much support in the human literature so far, there’s quite a bit of evidence for it in the animal literature. For example, when we want to produce obesity in rodents we typically use diets that are composed of refined ingredients, high in fat (40-60% of calories), contain some sugar (~10% of calories), and are highly palatable. These diets are extremely fattening in susceptible strains, but their fattening ability is only partially dependent on increased calorie intake. If you restrict an animal's energy intake so that it’s the same as rodents on a non-fattening unrefined diet (called ‘pair feeding’), they still gain most of the fat that they would have if you hadn’t restricted energy intake at all (14, 15)! This suggests that these diets make their bodies ‘want’ to be fat, and they will accomplish this goal by increasing calorie intake and/or by decreasing energy expenditure. This is related in large part to changes that occur in the brains of these animals (16).
The Study
Enter the recent study by Dr. David Ludwig’s group (1). This is a really fascinating, some might say groundbreaking, study. Although we know that differences in dietary carbohydrate and fat content have little or no impact on energy expenditure during overfeeding, in weight-stable people, or during weight loss, we don’t know much about how these impact energy expenditure during weight maintenance after weight loss. Weight maintenance is critical because it’s where most people’s weight loss efforts fail.
Contrary to some of the claims I'm sure are being made about this study, it wasn’t actually designed to tell whether fat and carbohydrate per se influence energy expenditure. What they compared were three distinct dietary patterns that differed in carbohydrate, fat, protein, and other aspects of diet composition, although carbohydrate content was certainly a major difference between groups.
In this study, they started with overweight and obese volunteers who had lost an average of 14 percent of body weight using a low-calorie diet. Then they placed them on three different diets, which were precisely controlled by the investigators:
Does this support the idea that there is a ‘metabolic advantage’ to low-carbohydrate diets? Well, sort of. It doesn’t change the previous findings that the carbohydrate:fat ratio has little or no impact on energy expenditure during overfeeding, in weight stable people, or during weight loss, but it does suggest that a VLC dietary pattern has a metabolic advantage over a LF diet specifically in the context of weight maintenance after weight loss. It also suggests that a LGI diet has a smaller but still meaningful metabolic advantage in this setting, and that a LF diet are not very effective in this regard. It also opens a whole new can of worms for the research world, investigating the effects of diet quality on energy expenditure.
So should everyone eat a VLC diet for weight loss maintenance then? Not so fast. The VLC diet group experienced some troubling hormonal changes that seem to be pretty common with this kind of diet. There were three main negative changes. The first and perhaps most troubling was an increase in cortisol, a stress hormone that may contribute to serious health problems over the long term (17). The second was a decrease in thyroid hormone, which is something that has been observed repeatedly with this kind of diet. Many of the negative effects that some people develop on long-term VLC diets (constipation, lethargy, poor sleep, hair loss, irritability) could be related to low thyroid function. This doesn't seem to be as much of an issue with moderate carbohydrate restriction. The third was an increase in C-reactive protein (CRP), a marker of inflammation and heart attack risk. Although the paper and media reports make a big deal out of the increase in CRP, it looks quite small to me—I’m not convinced it’s biologically significant.
The low-fat diet came out looking pretty poor as well. Energy expenditure was lowest on this diet, and estimated insulin sensitivity was also lowest (although the caveat here is that they didn't directly measure insulin sensitivity). This is interesting because as they remarked in the paper, this is the dietary advice most people will receive from nutrition authorities. This adds to the evidence that eating a bunch of whole grain breads and pastas is probably not a great strategy for weight loss maintenance.
Overall, the LGI diet came out looking the best overall. It’s the least restrictive of the three, conferred a pretty good ‘metabolic advantage’, and was not associated with harmful hormonal changes. I think this kind of diet would be a reasonable choice for weight maintenance following fat loss. I’ve been skeptical of the glycemic index concept in the past, and I continue to be, because most controlled studies have shown that in isolation it has little or no impact on body weight or insulin sensitivity (18, 19). The LGI diet in this study did indeed have a low glycemic index, but since it differed from the other diets in many other ways, we can’t know whether the glycemic index per se was a relevant factor.
In any case, a diet that focuses on beans/lentils, meats, nuts, fruits, and vegetables at the expense of grains (particularly flours) may be a good choice for weight loss maintenance, and I think this squares well with research coming from other angles. That being said, there are some major caveats to this study that must be kept in mind:
1. Calories don’t matter at all, only diet composition matters.
2. Calories are the only thing that matters, and diet composition is irrelevant.
3. Calories matter, but diet composition may also play a role.
The first one is an odd position that is not very well populated. The second one has a lot of adherents in the research world, and there’s enough evidence to make a good case for it. It’s represented by the phrase ‘a calorie is a calorie’, i.e. all calories are equally fattening. #1 and #2 are both extreme positions, and as such they get a lot of attention. But the third group, although less vocal, may be closest to the truth.
A Little Background on Food Intake, Diet Composition and Energy Expenditure
The energy content of the human body is determined by the amount of energy coming in, minus the energy exiting—simple on paper. Since body fat is by far the main energy storage site in the body, it follows that the balance between energy intake and energy expenditure determines fat mass, and this has been experimentally confirmed many times. But here’s the catch—energy expenditure is not always constant. For example, we know that it increases as a person gains weight, and decreases when a person loses weight (2). The decrease in energy expenditure with weight loss is caused by two things, 1) a smaller body requires fewer calories for maintenance, 2) a decrease in leptin, which decreases the metabolic rate by acting in the brain (3).
Some people have suggested that the type of food we eat, not just the amount, influences energy expenditure, and in particular that this is related to the diet's carbohydrate content. In people who are not trying to lose weight (4, 5), or who are being overfed (6, 7), the carbohydrate:fat ratio in the diet has little or no detectable impact on energy expenditure, and if anything it favors carbohydrate, but could this be different during fat loss in people who start off overweight? This idea has been called the ‘metabolic advantage’, most notably attributed to the low-carbohydrate diet. The idea here is that you can lose fat eating the same number of calories if carbohydrate is kept low.
I’ve never really weighed in on this because it’s a topic of heated debate, and in any case it’s a fairly academic question. Why is it academic? Because previous weight loss studies have shown that if a metabolic advantage exists at all, it’s quite small, because the effect is undetectable in most studies (8, 9, 10). People who are not associated with the low-carbohydrate community tend to conclude that there's no metabolic advantage when they review the literature (11), although I haven't reviewed it closely myself. It’s clear that where fat loss is concerned, calorie intake is much more important than the amount of fat or carbohydrate in the diet. What previous studies have suggested is that low-carbohydrate diets suppress appetite — often resulting in lower calorie intake (12, 13). The reason for this remains a topic of speculation.
That being said, I’m actually quite open to the idea that food quality in addition to quantity can influence body fatness, and I would encourage people to think outside the macronutrient box: there are probably many different dietary factors that can have such an effect. Although this idea hasn’t received much support in the human literature so far, there’s quite a bit of evidence for it in the animal literature. For example, when we want to produce obesity in rodents we typically use diets that are composed of refined ingredients, high in fat (40-60% of calories), contain some sugar (~10% of calories), and are highly palatable. These diets are extremely fattening in susceptible strains, but their fattening ability is only partially dependent on increased calorie intake. If you restrict an animal's energy intake so that it’s the same as rodents on a non-fattening unrefined diet (called ‘pair feeding’), they still gain most of the fat that they would have if you hadn’t restricted energy intake at all (14, 15)! This suggests that these diets make their bodies ‘want’ to be fat, and they will accomplish this goal by increasing calorie intake and/or by decreasing energy expenditure. This is related in large part to changes that occur in the brains of these animals (16).
The Study
Enter the recent study by Dr. David Ludwig’s group (1). This is a really fascinating, some might say groundbreaking, study. Although we know that differences in dietary carbohydrate and fat content have little or no impact on energy expenditure during overfeeding, in weight-stable people, or during weight loss, we don’t know much about how these impact energy expenditure during weight maintenance after weight loss. Weight maintenance is critical because it’s where most people’s weight loss efforts fail.
Contrary to some of the claims I'm sure are being made about this study, it wasn’t actually designed to tell whether fat and carbohydrate per se influence energy expenditure. What they compared were three distinct dietary patterns that differed in carbohydrate, fat, protein, and other aspects of diet composition, although carbohydrate content was certainly a major difference between groups.
In this study, they started with overweight and obese volunteers who had lost an average of 14 percent of body weight using a low-calorie diet. Then they placed them on three different diets, which were precisely controlled by the investigators:
- A low-fat (LF) diet “designed to reflect conventional recommendations to reduce dietary fat, emphasize whole grain products, and include a variety of vegetables and fruits”. 60-20-20 carbohydrate-fat-protein. I think these people were eating a lot of breads, pastas, etc.
- A low glycemic index (LGI) diet diet designed to “achieve a moderate glycemic load by replacing some grain products and starchy vegetables with sources of healthful fat and low–glycemic index vegetables, legumes, and fruits”. 40-40-20 carbohydrate-fat-protein. Low glycemic index carbohydrates are those that increase blood sugar less per unit carbohydrate eaten, such as beans, oatmeal, fruit, and sweet potatoes.
- A very low carbohydrate (VLC) diet that was “modeled on the Atkins Diet and had a low glycemic load due to more severe restriction of carbohydrate”. 10-60-30 carbohydrate-fat-protein. This is mostly meat, vegetables, eggs, nuts, and added fats. They also took a fiber supplement as recommended by Atkins.
Does this support the idea that there is a ‘metabolic advantage’ to low-carbohydrate diets? Well, sort of. It doesn’t change the previous findings that the carbohydrate:fat ratio has little or no impact on energy expenditure during overfeeding, in weight stable people, or during weight loss, but it does suggest that a VLC dietary pattern has a metabolic advantage over a LF diet specifically in the context of weight maintenance after weight loss. It also suggests that a LGI diet has a smaller but still meaningful metabolic advantage in this setting, and that a LF diet are not very effective in this regard. It also opens a whole new can of worms for the research world, investigating the effects of diet quality on energy expenditure.
So should everyone eat a VLC diet for weight loss maintenance then? Not so fast. The VLC diet group experienced some troubling hormonal changes that seem to be pretty common with this kind of diet. There were three main negative changes. The first and perhaps most troubling was an increase in cortisol, a stress hormone that may contribute to serious health problems over the long term (17). The second was a decrease in thyroid hormone, which is something that has been observed repeatedly with this kind of diet. Many of the negative effects that some people develop on long-term VLC diets (constipation, lethargy, poor sleep, hair loss, irritability) could be related to low thyroid function. This doesn't seem to be as much of an issue with moderate carbohydrate restriction. The third was an increase in C-reactive protein (CRP), a marker of inflammation and heart attack risk. Although the paper and media reports make a big deal out of the increase in CRP, it looks quite small to me—I’m not convinced it’s biologically significant.
The low-fat diet came out looking pretty poor as well. Energy expenditure was lowest on this diet, and estimated insulin sensitivity was also lowest (although the caveat here is that they didn't directly measure insulin sensitivity). This is interesting because as they remarked in the paper, this is the dietary advice most people will receive from nutrition authorities. This adds to the evidence that eating a bunch of whole grain breads and pastas is probably not a great strategy for weight loss maintenance.
Overall, the LGI diet came out looking the best overall. It’s the least restrictive of the three, conferred a pretty good ‘metabolic advantage’, and was not associated with harmful hormonal changes. I think this kind of diet would be a reasonable choice for weight maintenance following fat loss. I’ve been skeptical of the glycemic index concept in the past, and I continue to be, because most controlled studies have shown that in isolation it has little or no impact on body weight or insulin sensitivity (18, 19). The LGI diet in this study did indeed have a low glycemic index, but since it differed from the other diets in many other ways, we can’t know whether the glycemic index per se was a relevant factor.
In any case, a diet that focuses on beans/lentils, meats, nuts, fruits, and vegetables at the expense of grains (particularly flours) may be a good choice for weight loss maintenance, and I think this squares well with research coming from other angles. That being said, there are some major caveats to this study that must be kept in mind:
- It was only four weeks long. We don't know if this difference would have continued in the long run.
- The study was not designed to measure long-term changes in fat mass, which is what we're ultimately interested in.
- This was done under calorie-controlled conditions, not under free-living conditions as most people would apply these diets. Under free-living conditions, the main determinant of long-term fat loss seems to be how well you stick to a diet, not which diet you choose (20, 21, 22).
- There was a lot of individual variability in this study, confirming once again that everyone is different. There is no reason to stick to a diet if it's not working for you, just because a study says it works well for the "average person". Kudos to Drs. Ebbeling and Ludwig for reporting individual data.
Kaydol:
Yorumlar (Atom)